Interfaculty Initiative in Health Policy, Harvard Graduate School of Arts and Sciences, Cambridge, Massachusetts (A.B.).
Center for Health Policy and Center for Primary Care and Outcomes Research, Stanford University School of Medicine, Stanford, California (J.A.S.).
Ann Intern Med. 2021 Aug;174(8):1090-1100. doi: 10.7326/M21-0600. Epub 2021 Jun 8.
The COVID-19 pandemic has induced historic educational disruptions. In April 2021, about 40% of U.S. public school students were not offered full-time in-person education.
To assess the risk for SARS-CoV-2 transmission in schools.
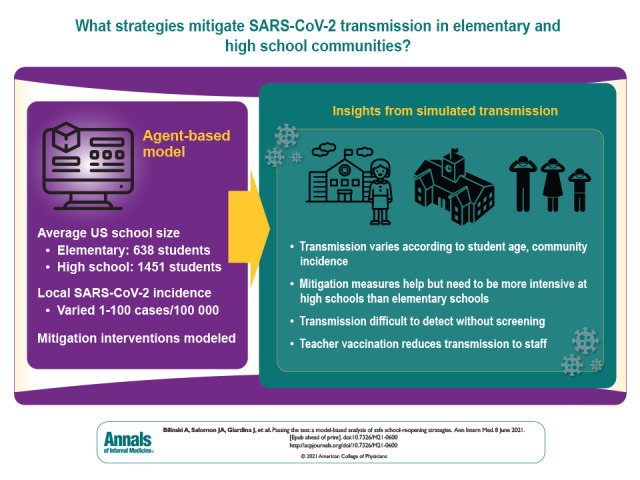
An agent-based network model was developed to simulate transmission in elementary and high school communities, including home, school, and interhousehold interactions.
School structure was parametrized to reflect average U.S. classrooms, with elementary schools of 638 students and high schools of 1451 students. Daily local incidence was varied from 1 to 100 cases per 100 000 persons.
Students, faculty, staff, and adult household members.
Isolation of symptomatic individuals, quarantine of an infected individual's contacts, reduced class sizes, alternative schedules, staff vaccination, and weekly asymptomatic screening.
Transmission was projected among students, staff, and families after a single infection in school and over an 8-week quarter, contingent on local incidence.
School transmission varies according to student age and local incidence and is substantially reduced with mitigation measures. Nevertheless, when transmission occurs, it may be difficult to detect without regular testing because of the subclinical nature of most children's infections. Teacher vaccination can reduce transmission to staff, and asymptomatic screening improves understanding of local circumstances and reduces transmission.
Uncertainty exists about the susceptibility and infectiousness of children, and precision is low regarding the effectiveness of specific countermeasures, particularly with new variants.
With controlled community transmission and moderate mitigation, elementary schools can open safety, but high schools require more intensive mitigation. Asymptomatic screening can facilitate reopening at higher local incidence while minimizing transmission risk.
Centers for Disease Control and Prevention through the Council of State and Territorial Epidemiologists, National Institute of Allergy and Infectious Diseases, National Institute on Drug Abuse, and Facebook.
COVID-19 大流行导致了历史性的教育中断。2021 年 4 月,约 40%的美国公立学校学生没有接受全日制面授教育。
评估学校中 SARS-CoV-2 传播的风险。
开发了一个基于代理的网络模型,以模拟小学和高中社区(包括家庭、学校和家庭之间的互动)中的传播。
学校结构参数化,以反映美国普通教室,小学 638 名学生,高中 1451 名学生。每日当地发病率从每 10 万人 1 到 100 例不等。
学生、教师、工作人员和成年家庭成员。
隔离症状患者、隔离感染患者的接触者、减少班级规模、交替时间表、员工接种疫苗和每周无症状筛查。
在学校发生单次感染后,并在 8 周的季度中,根据当地发病率,预测学生、教职员工和家庭之间的传播情况。
学校传播因学生年龄和当地发病率而异,通过缓解措施可显著降低。然而,由于大多数儿童感染呈亚临床状态,因此如果没有定期检测,传播可能难以发现。教师接种疫苗可以减少对员工的传播,无症状筛查可以更好地了解当地情况并降低传播风险。
儿童的易感性和传染性存在不确定性,特定对策的有效性精度较低,尤其是新变体。
在社区传播得到控制且缓解措施适度的情况下,小学可以安全开放,但高中需要更严格的缓解措施。无症状筛查可以在更高的当地发病率下促进重新开放,同时最大限度地降低传播风险。
疾病控制与预防中心通过州和地区流行病学家理事会、国家过敏和传染病研究所、国家药物滥用研究所和 Facebook。