Dipartimento Di Scienze Biotecnologiche Di Base, Cliniche Intensivologiche E Perioperatorie, Università Cattolica del Sacro Cuore, Rome, Italy.
Dipartimento Di Scienze Dell'Emergenza, Anestesiologiche e della Rianimazione, Fondazione Policlinico Universitario A. Gemelli IRCCS - Università Cattolica del Sacro Cuore Largo A. Gemelli 8, 00168, Rome, Italy.
Crit Care. 2021 Jun 7;25(1):197. doi: 10.1186/s13054-021-03623-4.
Hospitalized patients with COVID-19 admitted to the intensive care unit (ICU) and requiring mechanical ventilation are at risk of ventilator-associated bacterial infections secondary to SARS-CoV-2 infection. Our study aimed to investigate clinical features of Staphylococcus aureus ventilator-associated pneumonia (SA-VAP) and, if bronchoalveolar lavage samples were available, lung bacterial community features in ICU patients with or without COVID-19.
We prospectively included hospitalized patients with COVID-19 across two medical ICUs of the Fondazione Policlinico Universitario A. Gemelli IRCCS (Rome, Italy), who developed SA-VAP between 20 March 2020 and 30 October 2020 (thereafter referred to as cases). After 1:2 matching based on the simplified acute physiology score II (SAPS II) and the sequential organ failure assessment (SOFA) score, cases were compared with SA-VAP patients without COVID-19 (controls). Clinical, microbiological, and lung microbiota data were analyzed.
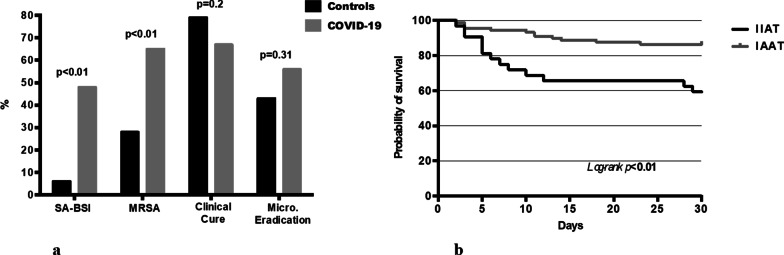
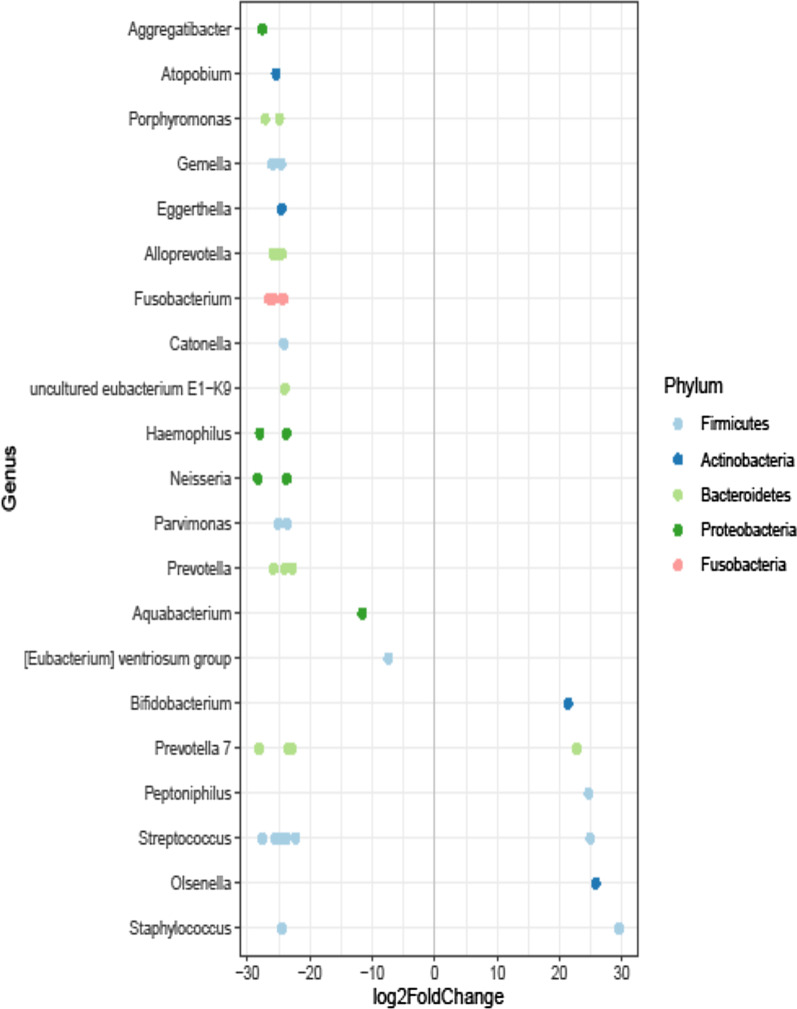
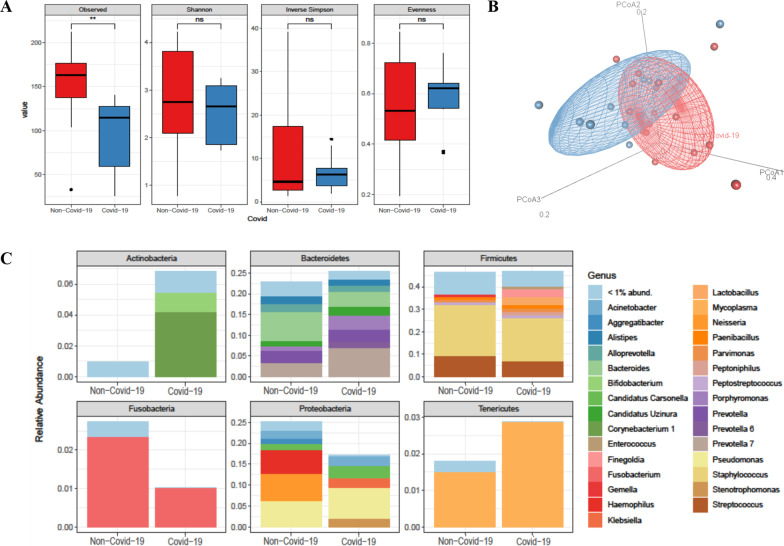
We studied two groups of patients (40 COVID-19 and 80 non-COVID-19). COVID-19 patients had a higher rate of late-onset (87.5% versus 63.8%; p = 0.01), methicillin-resistant (65.0% vs 27.5%; p < 0.01) or bacteremic (47.5% vs 6.3%; p < 0.01) infections compared with non-COVID-19 patients. No statistically significant differences between the patient groups were observed in ICU mortality (p = 0.12), clinical cure (p = 0.20) and microbiological eradication (p = 0.31). On multivariable logistic regression analysis, SAPS II and initial inappropriate antimicrobial therapy were independently associated with ICU mortality. Then, lung microbiota characterization in 10 COVID-19 and 16 non-COVID-19 patients revealed that the overall microbial community composition was significantly different between the patient groups (unweighted UniFrac distance, R 0.15349; p < 0.01). Species diversity was lower in COVID-19 than in non COVID-19 patients (94.4 ± 44.9 vs 152.5 ± 41.8; p < 0.01). Interestingly, we found that S. aureus (log fold change, 29.5), Streptococcus anginosus subspecies anginosus (log fold change, 24.9), and Olsenella (log fold change, 25.7) were significantly enriched in the COVID-19 group compared to the non-COVID-19 group of SA-VAP patients.
In our study population, COVID-19 seemed to significantly affect microbiological and clinical features of SA-VAP as well as to be associated with a peculiar lung microbiota composition.
因 SARS-CoV-2 感染而入住重症监护病房(ICU)并需要机械通气的 COVID-19 住院患者存在发生与呼吸机相关的细菌感染(VAP)的风险。本研究旨在调查 ICU 中 COVID-19 患者与非 COVID-19 患者的金黄色葡萄球菌 VAP(SA-VAP)的临床特征,以及如果有支气管肺泡灌洗样本,其肺部细菌群落特征。
我们前瞻性纳入了意大利罗马 Gemelli 大学附属 Policlinico 基金会 A. Gemelli 综合医院(Fondazione Policlinico Universitario A. Gemelli IRCCS)两个医学 ICU 中于 2020 年 3 月 20 日至 2020 年 10 月 30 日期间发生 SA-VAP 的 COVID-19 住院患者(此后称为病例)。在基于简化急性生理学评分 II(SAPS II)和序贯器官衰竭评估(SOFA)评分进行 1:2 匹配后,将病例与没有 COVID-19 的 SA-VAP 患者(对照组)进行比较。分析了临床、微生物学和肺部微生物组数据。
我们研究了两组患者(COVID-19 患者 40 例,非 COVID-19 患者 80 例)。与非 COVID-19 患者相比,COVID-19 患者的晚发性(87.5% 比 63.8%;p=0.01)、耐甲氧西林(65.0% 比 27.5%;p<0.01)或菌血症(47.5% 比 6.3%;p<0.01)感染的发生率更高。两组患者在 ICU 死亡率(p=0.12)、临床治愈率(p=0.20)和微生物学清除率(p=0.31)方面无统计学差异。多变量逻辑回归分析显示,SAPS II 和初始不适当的抗菌治疗与 ICU 死亡率独立相关。然后,对 10 例 COVID-19 患者和 16 例非 COVID-19 患者的肺部微生物组特征进行分析,结果显示两组患者的整体微生物群落组成存在显著差异(非加权 UniFrac 距离,R 0.15349;p<0.01)。COVID-19 患者的物种多样性低于非 COVID-19 患者(94.4±44.9 比 152.5±41.8;p<0.01)。有趣的是,我们发现与非 COVID-19 组的 SA-VAP 患者相比,金黄色葡萄球菌(log 倍数变化,29.5)、咽峡炎链球菌亚种咽峡炎链球菌(log 倍数变化,24.9)和奥尔森菌(log 倍数变化,25.7)在 COVID-19 组中明显富集。
在我们的研究人群中,COVID-19 似乎显著影响了 SA-VAP 的微生物学和临床特征,并与肺部特定的微生物群落组成有关。