Department of Pneumology, Arnaud de Villeneuve, Regional University Hospital of Montpellier, Montpellier, France.
PhyMedExp, University of Montpellier, INSERM U1046, CNRS UMR 9214, Montpellier, France.
ESC Heart Fail. 2021 Aug;8(4):2513-2526. doi: 10.1002/ehf2.13455. Epub 2021 Jun 8.
Optimizing medical cardiac treatment for sleep apnoea (SA) in patients with chronic heart failure and reduced ejection fraction (HFrEF) is an expert Grade C recommendation based on six studies encompassing a total of 67 patients only. Whether sacubitril-valsartan (SV), a cornerstone of HFrEF medical treatment, impacts SA is unknown and requires evaluation.
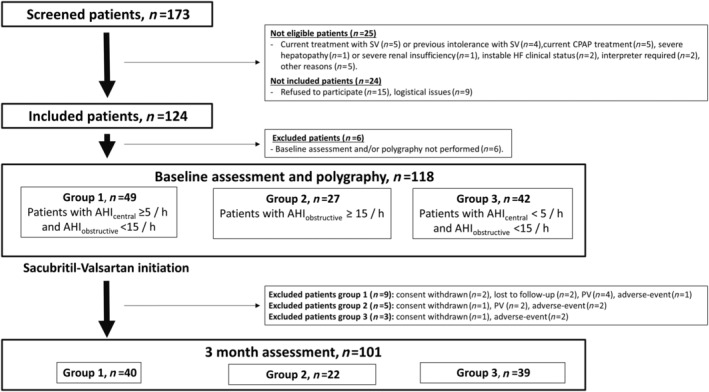
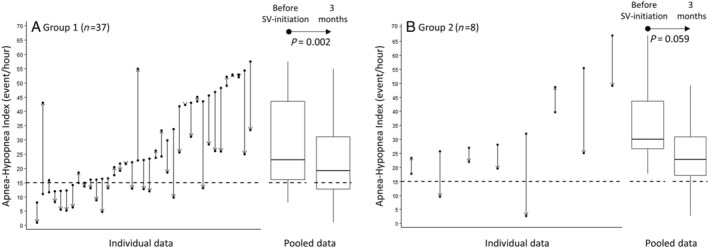
The ENTRESTO-SAS trial is a six-centre, prospective, open-label real-life cohort study (NCT02916160). Ambulatory patients eligible for SV (i.e. HFrEF adults who remain symptomatic despite optimal treatment) were evaluated before and after 3 months of SV (including nocturnal ventilatory polygraphy); 118 patients were final analysed [median age was 66 (IQ : 56-73) years, 81.4% male, 36.5% New York Heart Association III-IV, N-terminal pro-B-type natriuretic peptide level of 1564 (701-3376) ng/L, left ventricular ejection fraction of 30 (25-34)%, 60.7% ischaemic HFrEF, 97.5% initially treated with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, 83.9% with beta-blockers, 64.4% with mineralocorticoid receptor antagonists, and 74.6% with diuretics]. Three groups were defined according to initial central/obstructive apnoea-hypopnoea indices (AHIs): G1 (n = 49, AHI ≥ 5/h and AHI < 15/h); G2 (n = 27, AHI ≥ 15/h); and G3 (n = 42, AHI < 5/h and AHI < 15/h). At 3 months, the AHI (main predefined outcome) decreased significantly by -7.10/h (IQ : -16.10 to 0.40; P < 0.001) in G1 + G2 without positive airway pressure treatment (45 patients, median initial AHI of 24.20 (IQ : 16.40-43.50)/h). Of these, 24.4% presented an AHI decrease ≥50% and 37.78% had a final AHI < 15/h (tendency for improvement from an initial value of 20%: P = 0.0574). For G1 patients (n = 37), AHI significantly decreased from a median of 22.90 (16.00-43.50)/h to 19.20 (12.70-31.10)/h (P = 0.002). For G2 patients (n = 8), AHI decreased from a median of 30.10 (26.40-47.60)/h to 22.75 (14.60-36.90)/h (statistically non-significant, P = 0.059).
In this real-life population, SV treatment for 3 months in SA patients is associated with a significant decrease in AHI. These results support the current guidelines that recommend first an optimization of the HFrEF treatment in patients with HFrEF and central SA. A potential positive airway pressure sparing effect merits further investigation.
对于射血分数降低的心力衰竭(HFrEF)合并睡眠呼吸暂停(SA)的患者,优化心脏治疗方案是专家 C 级推荐,基于仅有六项研究涵盖了总共 67 名患者。沙库巴曲缬沙坦(SV)是否会影响 SA,目前尚不清楚,需要进一步评估。
ENTRESTO-SAS 试验是一项六中心、前瞻性、开放标签的真实世界队列研究(NCT02916160)。有资格接受 SV 治疗(即仍有症状的 HFrEF 成人,尽管接受了最佳治疗)的门诊患者在接受 SV 治疗前后 3 个月进行了评估(包括夜间通气多导睡眠图);最终分析了 118 名患者[中位年龄为 66(IQ:56-73)岁,81.4%为男性,36.5%为纽约心脏协会 III-IV 级,N 末端脑利钠肽前体水平为 1564(701-3376)ng/L,左心室射血分数为 30(25-34)%,60.7%为缺血性 HFrEF,97.5%最初接受血管紧张素转换酶抑制剂或血管紧张素 II 受体阻滞剂治疗,83.9%接受β受体阻滞剂治疗,64.4%接受盐皮质激素受体拮抗剂治疗,74.6%接受利尿剂治疗]。根据初始中枢性/阻塞性呼吸暂停低通气指数(AHI)将患者分为三组:G1 组(n=49,AHI≥5/h 且 AHI<15/h);G2 组(n=27,AHI≥15/h);G3 组(n=42,AHI<5/h 且 AHI<15/h)。3 个月时,AHI(主要预设结局)在未接受正压通气治疗的 G1+G2 患者中显著下降了-7.10/h(IQ:-16.10 至 0.40;P<0.001)(45 名患者,中位初始 AHI 为 24.20(IQ:16.40-43.50)/h)。其中,24.4%的患者 AHI 下降≥50%,37.78%的患者最终 AHI<15/h(初始值改善的趋势:P=0.0574)。对于 G1 患者(n=37),AHI 从中位数 22.90(16.00-43.50)/h 显著下降至 19.20(12.70-31.10)/h(P=0.002)。对于 G2 患者(n=8),AHI 从中位数 30.10(26.40-47.60)/h 下降至 22.75(14.60-36.90)/h(统计学上无显著差异,P=0.059)。
在这项真实世界的研究中,SA 患者接受 SV 治疗 3 个月后,AHI 显著下降。这些结果支持目前的指南,建议首先优化 HFrEF 合并中枢性 SA 患者的 HFrEF 治疗方案。可能存在正压通气保留作用,值得进一步研究。