Maggs Luke, Cattaneo Giulia, Dal Ali Emre, Moghaddam Ali Sanjari, Ferrone Soldano
Department of Surgery, Massachusetts General Hospital and Harvard Medical School, Boston, MA, United States.
Front Neurosci. 2021 May 25;15:662064. doi: 10.3389/fnins.2021.662064. eCollection 2021.
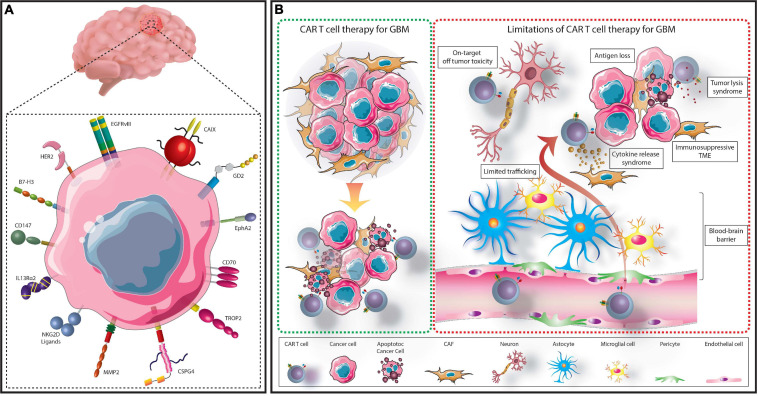
Glioblastoma multiforme (GBM) is the most common and aggressive malignant primary brain tumor in adults. Current treatment options typically consist of surgery followed by chemotherapy or more frequently radiotherapy, however, median patient survival remains at just over 1 year. Therefore, the need for novel curative therapies for GBM is vital. Characterization of GBM cells has contributed to identify several molecules as targets for immunotherapy-based treatments such as EGFR/EGFRvIII, IL13Rα2, B7-H3, and CSPG4. Cytotoxic T lymphocytes collected from a patient can be genetically modified to express a chimeric antigen receptor (CAR) specific for an identified tumor antigen (TA). These CAR T cells can then be re-administered to the patient to identify and eliminate cancer cells. The impressive clinical responses to TA-specific CAR T cell-based therapies in patients with hematological malignancies have generated a lot of interest in the application of this strategy with solid tumors including GBM. Several clinical trials are evaluating TA-specific CAR T cells to treat GBM. Unfortunately, the efficacy of CAR T cells against solid tumors has been limited due to several factors. These include the immunosuppressive tumor microenvironment, inadequate trafficking and infiltration of CAR T cells and their lack of persistence and activity. In particular, GBM has specific limitations to overcome including acquired resistance to therapy, limited diffusion across the blood brain barrier and risks of central nervous system toxicity. Here we review current CAR T cell-based approaches for the treatment of GBM and summarize the mechanisms being explored in pre-clinical, as well as clinical studies to improve their anti-tumor activity.
多形性胶质母细胞瘤(GBM)是成人中最常见且侵袭性最强的原发性恶性脑肿瘤。目前的治疗方案通常包括手术,随后进行化疗,或更常见的是放疗,然而,患者的中位生存期仍仅略超过1年。因此,迫切需要针对GBM的新型治愈性疗法。对GBM细胞的特征描述有助于确定几种分子作为基于免疫疗法的治疗靶点,如表皮生长因子受体/表皮生长因子受体变异体III(EGFR/EGFRvIII)、白细胞介素13受体α2(IL13Rα2)、B7-H3和硫酸软骨素蛋白聚糖4(CSPG4)。从患者体内收集的细胞毒性T淋巴细胞可通过基因改造来表达针对已确定肿瘤抗原(TA)的嵌合抗原受体(CAR)。然后可将这些CAR T细胞重新注入患者体内以识别和清除癌细胞。基于TA特异性CAR T细胞的疗法在血液系统恶性肿瘤患者中取得了令人瞩目的临床反应,这引发了人们对将该策略应用于包括GBM在内的实体瘤的浓厚兴趣。多项临床试验正在评估TA特异性CAR T细胞治疗GBM的效果。不幸的是,由于多种因素,CAR T细胞对实体瘤的疗效受到了限制。这些因素包括免疫抑制性肿瘤微环境、CAR T细胞的运输和浸润不足以及它们缺乏持久性和活性。特别是,GBM有特定的局限性需要克服,包括对治疗产生获得性耐药、穿过血脑屏障的扩散有限以及中枢神经系统毒性风险。在此,我们综述了目前基于CAR T细胞治疗GBM的方法,并总结了临床前以及临床研究中正在探索的改善其抗肿瘤活性的机制。