Division of Nephrology, University of Toronto, Toronto, Ontario, Canada.
Division of Endocrinology, Diabetes and Metabolism, University of Tennessee Health Science Center, Memphis, Tennessee, USA.
Clin Cardiol. 2021 Aug;44(8):1139-1143. doi: 10.1002/clc.23665. Epub 2021 Jun 15.
A recent meta-analysis of sodium-glucose cotransporter 2 (SGLT2) inhibitor outcome trials reported that SGLT2 inhibitors were associated with reduction in the risk of adverse composite kidney outcomes, with moderate heterogeneity across the trials; however, the endpoints were defined differently across the trials.
The apparent heterogeneity of the meta-analysis of kidney composite outcomes of SGLT2 inhibitor trials will be substantially reduced by using a consistent assessment of sustained ≥40% decline in eGFR/chronic kidney dialysis/transplantation/renal death across trials.
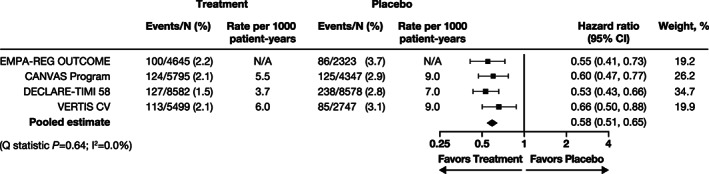
We performed a meta-analysis of kidney composite outcomes from the four SGLT2 cardiovascular outcome trial programs conducted in general type 2 diabetes mellitus populations, which included, as a surrogate of progression to kidney failure, a sustained ≥40% decline in eGFR along with kidney replacement therapy and kidney death. The trials assessed were VERTIS CV (NCT01986881), CANVAS Program (NCT01032629 and NCT01989754), DECLARE-TIMI 58 (NCT01730534), and EMPA-REG OUTCOME (NCT01131676).
Data from the trials comprised 42 516 individual participants; overall, 998 composite kidney events occurred. SGLT2 inhibition was associated with a significant reduction in the kidney composite endpoint (HR 0.58 [95% CI 0.51-0.65]) and with a highly consistent effect across the trials (Q statistic p = .64; I = 0.0%).
Our meta-analysis highlights the value of using similarly defined endpoints across trials and supports the finding of consistent protection against kidney disease progression with SGLT2 inhibitors as a class in patients with type 2 diabetes mellitus who either have established atherosclerotic cardiovascular disease or are at high cardiovascular risk with multiple cardiovascular risk factors.
最近对钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂结局试验的荟萃分析报告称,SGLT2 抑制剂与降低不良复合肾脏结局的风险相关,各试验之间存在中度异质性;然而,各试验的终点定义不同。
通过使用一致的评估方法,即各试验中 eGFR 持续下降≥40%、慢性肾脏透析/移植/肾脏死亡,可显著降低 SGLT2 抑制剂试验肾脏复合结局荟萃分析的明显异质性。
我们对四项在一般 2 型糖尿病患者人群中进行的 SGLT2 心血管结局试验计划的肾脏复合结局进行了荟萃分析,其中包括 eGFR 持续下降≥40%以及肾脏替代治疗和肾脏死亡作为进展为肾衰竭的替代指标。评估的试验包括 VERTIS CV(NCT01986881)、CANVAS 计划(NCT01032629 和 NCT01989754)、DECLARE-TIMI 58(NCT01730534)和 EMPA-REG OUTCOME(NCT01131676)。
来自试验的数据包含 42516 名个体参与者;总体上,发生了 998 例复合肾脏事件。SGLT2 抑制与肾脏复合终点显著降低相关(HR 0.58[95%CI 0.51-0.65]),并且在各试验中具有高度一致的效果(Q 统计量 p=0.64;I ²=0.0%)。
我们的荟萃分析强调了在各试验中使用类似定义的终点的价值,并支持 SGLT2 抑制剂作为一类药物在既有动脉粥样硬化性心血管疾病或存在多种心血管危险因素的高危心血管风险的 2 型糖尿病患者中一致保护肾脏疾病进展的发现。