Department of Surgery, University of Maryland School of Medicine, Baltimore, Maryland; Surgery Service, Veterans Affairs Medical Centre, Baltimore, Maryland.
Department of Surgery, University of Maryland School of Medicine, Baltimore, Maryland.
J Surg Res. 2021 Nov;267:211-216. doi: 10.1016/j.jss.2021.05.028. Epub 2021 Jun 19.
The COVID-19 pandemic has resulted in over 225,000 excess deaths in the United States. A moratorium on elective surgery was placed early in the pandemic to reduce risk to patients and staff and preserve critical care resources. This report evaluates the impact of the elective surgical moratorium on case volumes and intensive care unit (ICU) bed utilization.
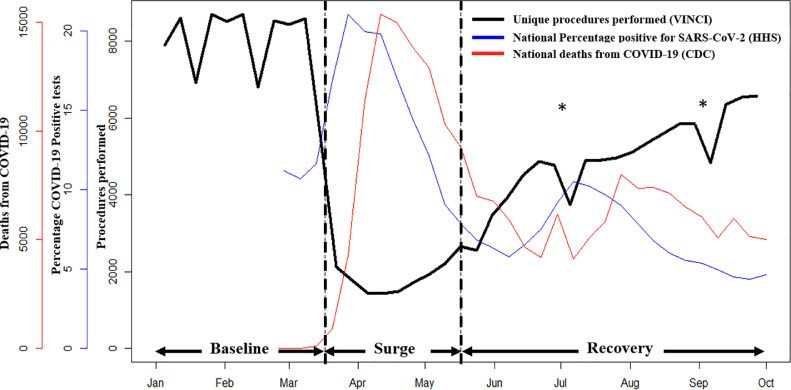
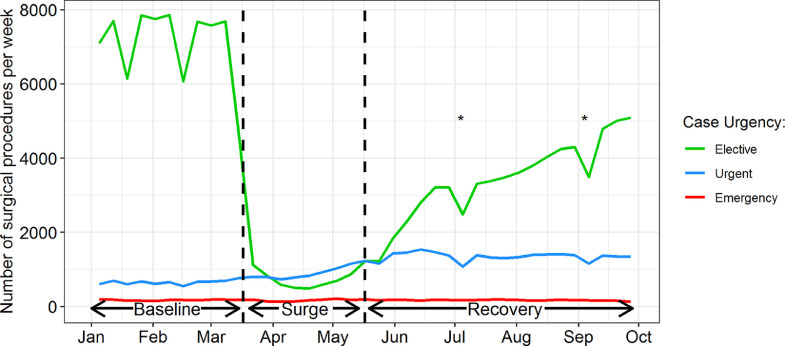
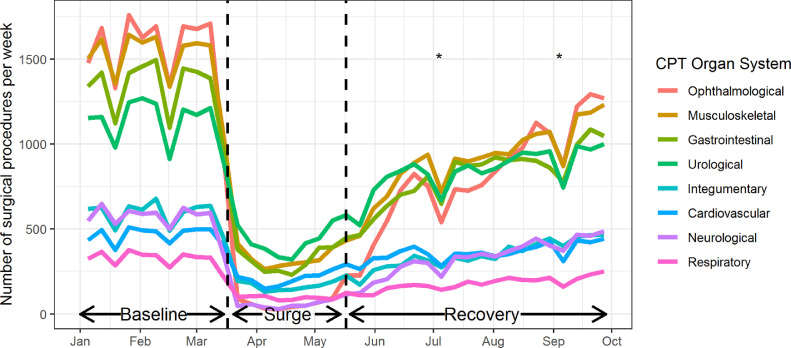
This retrospective review used a national convenience sample to correlate trends in the weekly rates of surgical cases at 170 Veterans Affairs Hospitals around the United States from January 1 to September 30, 2020 to national trends in the COVID-19 pandemic. We reviewed data on weekly number of procedures performed and ICU bed usage, stratified by level of urgency (elective, urgent, emergency), and whether an ICU bed was required within 24 hours of surgery. National data on the proportion of COVID-19 positive test results and mortality rates were obtained from the Center for Disease Control website.
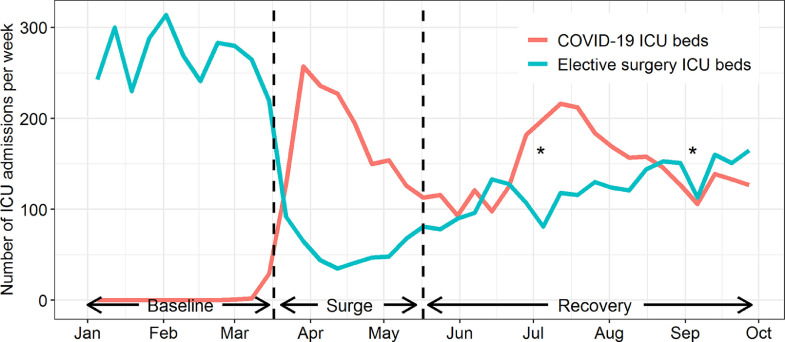
198,911 unique surgical procedures performed during the study period. The total number of cases performed from January 1 to March 16 was 86,004 compared with 15,699 from March 17 to May 17. The reduction in volume occurred before an increase in the percentage of COVID-19 positive test results and deaths nationally. There was a 91% reduction from baseline in the number of elective surgeries performed allowing 78% of surgical ICU beds to be available for COVID-19 positive patients.
The moratorium on elective surgical cases was timely and effective in creating bed capacity for critically ill COVID-19 patients. Further analyses will allow targeted resource allocation for future pandemic planning.
COVID-19 大流行导致美国超过 22.5 万人超额死亡。大流行早期,美国暂停了择期手术,以降低患者和医护人员的风险,并保护重症监护资源。本报告评估了择期手术暂停对手术量和重症监护病房(ICU)床位使用的影响。
本回顾性研究使用全国便利样本,将 2020 年 1 月 1 日至 9 月 30 日期间美国 170 家退伍军人事务医院每周手术病例的发生率趋势与 COVID-19 大流行期间的全国趋势相关联。我们回顾了每周手术数量和 ICU 床位使用的数据,按紧急程度(择期、紧急、急诊)分层,并分析是否需要在手术 24 小时内使用 ICU 床位。从疾病控制中心网站获取全国 COVID-19 阳性检测结果比例和死亡率的数据。
研究期间共进行了 198911 例独特的手术。从 1 月 1 日至 3 月 16 日共进行了 86004 例手术,而从 3 月 17 日至 5 月 17 日则进行了 15699 例手术。手术量的减少发生在全国 COVID-19 阳性检测结果和死亡人数增加之前。与基线相比,择期手术数量减少了 91%,使 78%的外科 ICU 床位可用于 COVID-19 阳性患者。
暂停择期手术及时有效地为重症 COVID-19 患者创造了床位容量。进一步的分析将允许为未来的大流行规划进行有针对性的资源分配。