Kawanishi Koki, Ikeda Yoshifumi, Furotani Masahiko, Tsuboi Sayaka, Kanno Takayuki, Niwa Toru, Nagaoka Tsunehiro, Tabata Yoshinari, Kitano Masayuki
Department of Gastroenterology, Nate Hospital, Kinokawa City, Wakayama, Japan.
Department of General Surgery, Wakayama Seikyo Hospital, Wakayama City, Wakayama, Japan.
Oxf Med Case Reports. 2021 Jun 18;2021(6):omab033. doi: 10.1093/omcr/omab033. eCollection 2021 Jun.
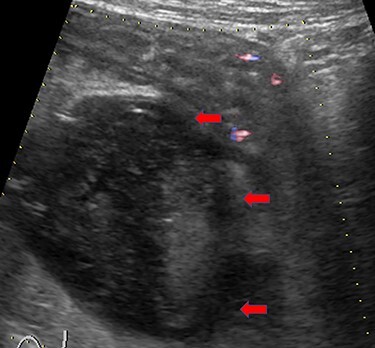
Intestinal anisakiasis is not only a rare but also a difficult to diagnose parasitic disease. The symptoms are not specific and are often severe and abrupt; therefore, patients are sometimes diagnosed as having surgical abdomen. The clinical imaging findings are remarkable, including ascites, enteritis, ileus, eosinophilic granuloma and sometimes perforation. We experienced a case of intestinal anisakiasis diagnosed on the basis of the -specific immunoglobulin A level from paired sera and treated successfully with conservative therapy, although ileum perforation was complicated by a 50-mm abscess. Even the large abscess could be treated without drainage in thiscase.
肠道异尖线虫病不仅是一种罕见的,而且是一种难以诊断的寄生虫病。其症状不具有特异性,往往严重且突发;因此,患者有时被诊断为急腹症。临床影像学表现显著,包括腹水、肠炎、肠梗阻、嗜酸性粒细胞肉芽肿,有时还会出现穿孔。我们遇到一例根据双份血清中特异性免疫球蛋白A水平诊断出的肠道异尖线虫病病例,尽管回肠穿孔并发了一个50毫米的脓肿,但通过保守治疗成功治愈。在这个病例中,即使是大脓肿也无需引流即可治愈。