Department of Maternal Fetal Medicine, KK Women's and Children's Hospital, Singapore, Singapore.
Division of Nursing, KK Women's and Children's Hospital, Singapore, Singapore.
J Obstet Gynaecol Res. 2021 Sep;47(9):3171-3178. doi: 10.1111/jog.14907. Epub 2021 Jun 23.
To compare the efficacy and safety of dinoprostone vaginal insert (DVI) alone versus DVI with adjunctive sweeping of membranes (ASM) for induction of labor (IOL).
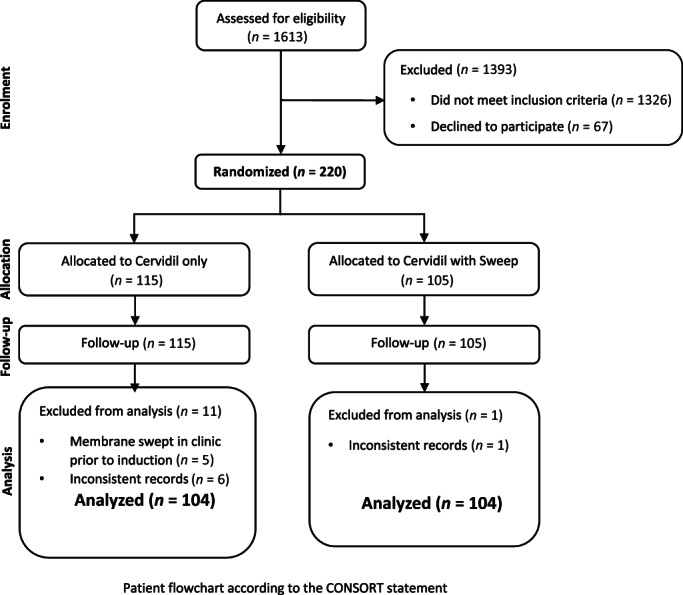
Single-center, prospective, randomized controlled trial; women with singleton term pregnancies, cervical dilation ≥1 and <3 cm, intact membranes allocated to either DVI or DVI with ASM. The primary outcome was vaginal delivery within 24 h of insertion. Secondary outcomes included mean time from insertion to delivery, tachysystole, operative delivery for non-reassuring fetal status (NRFS), tocolytics, fetal outcomes, pain information, and subject satisfaction.
One hundred and four received DVI (Group 1) alone and 104 DVI with ASM (Group 2). The rate of vaginal delivery within 24 h was 53% versus 56%, cesarean rate 8.7% versus 10.6% in Groups 1 and 2 respectively. Although the duration of labor was similar in both groups, about 6% of women required additional ripening with dinoprostone vaginal tablets in Group 2 compared to 11.5% in Group 1 (p-value = 0.2). The frequency of hyperstimulation syndrome, failed induction, analgesic requirements, and fetal outcomes were comparable. The majority (83%-86%) in either cohort were satisfied with their labor experience. Multivariate logistic regression demonstrated a slightly better chance for vaginal delivery within 24 h (odds ratio [OR] 1.22 [95% confidence interval, CI 0.65-2.29]; p-value 0.53] for DVI with ASM, although statistically insignificant. Younger maternal age and multiparity (OR 10.36 [95% CI 4.88-23.67]; p-value <0.0001) contributed to successful IOL.
DVI with ASM is at least as efficacious as DVI for cervical ripening with no increase in morbidity. Although DVI with ASM group less often needed additional dinoprostone tablets to complete the process of IOL (p-value = 0.2), adjunctive sweeping has not been shown to have a significant impact on the duration of labor or mode of delivery.
比较地诺前列酮阴道栓剂(DVI)单独使用与 DVI 联合胎膜剥膜术(ASM)用于引产(IOL)的疗效和安全性。
单中心、前瞻性、随机对照试验;纳入单胎足月妊娠、宫颈扩张 1~3cm、胎膜完整的孕妇,随机分为 DVI 组或 DVI 联合 ASM 组。主要结局为插入后 24 小时内阴道分娩。次要结局包括从插入到分娩的平均时间、宫缩过速、因非胎儿情况可接受(NRFS)行剖宫产、宫缩抑制剂、胎儿结局、疼痛信息和患者满意度。
104 例孕妇接受 DVI 单独使用(第 1 组),104 例孕妇 DVI 联合 ASM(第 2 组)。第 1 组和第 2 组 24 小时内阴道分娩率分别为 53%和 56%,剖宫产率分别为 8.7%和 10.6%。虽然两组的产程相似,但第 2 组约有 6%的孕妇需要额外使用地诺前列酮阴道片催产,而第 1 组为 11.5%(p 值=0.2)。过度刺激综合征、引产失败、镇痛需求和胎儿结局的发生率相似。两组中大多数(83%-86%)患者对分娩经历满意。多变量逻辑回归显示,DVI 联合 ASM 组 24 小时内阴道分娩的机会略有增加(优势比[OR]1.22[95%置信区间,CI 0.65-2.29];p 值=0.53),但无统计学意义。产妇年龄较小和多胎妊娠(OR 10.36[95%CI 4.88-23.67];p 值<0.0001)有助于成功进行 IOL。
DVI 联合 ASM 与 DVI 单独使用相比,在宫颈成熟方面同样有效,且不会增加发病率。尽管 DVI 联合 ASM 组完成 IOL 过程中较少需要额外的地诺前列酮片(p 值=0.2),但辅助剥膜并没有显著影响产程或分娩方式。