Pulmonary Center, Boston University School of Medicine, Boston, Massachusetts, United States of America.
PLoS One. 2021 Jun 24;16(6):e0252206. doi: 10.1371/journal.pone.0252206. eCollection 2021.
Although both leukocytosis and leukopenia have been considered Systemic Inflammatory Response Syndrome criteria, leukopenia is not generally considered a normal response to infection. We sought to evaluate the prognostic validity of leukopenia as a sign of sepsis-defining hematological organ dysfunction within the Sepsis-3 framework. We hypothesized that leukopenia is associated with higher risk of mortality than leukocytosis among patients with suspected infection.
We performed a retrospective cohort study using the Medical Information Mart v1.4 in Intensive Care-III database. Multivariable regression models were used to evaluate the association between leukopenia and mortality in patients with suspected infection defined by Sepsis-3.
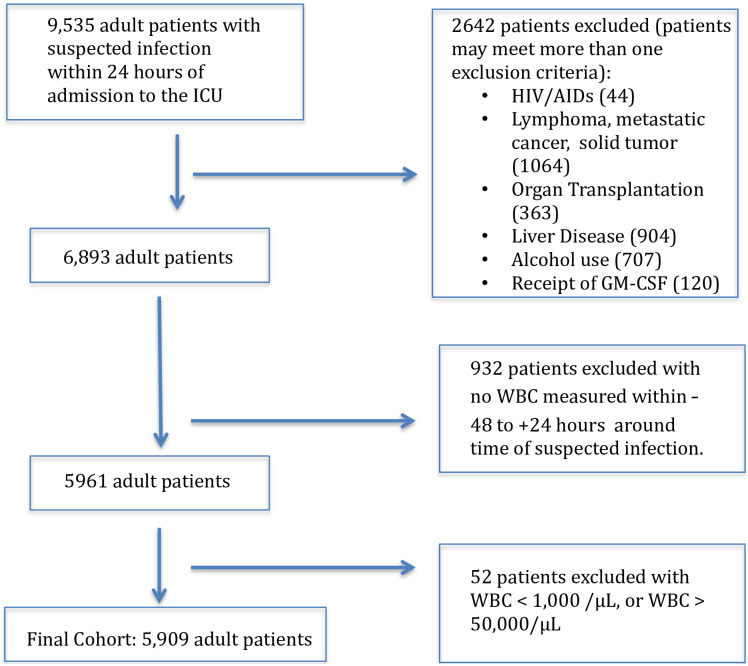
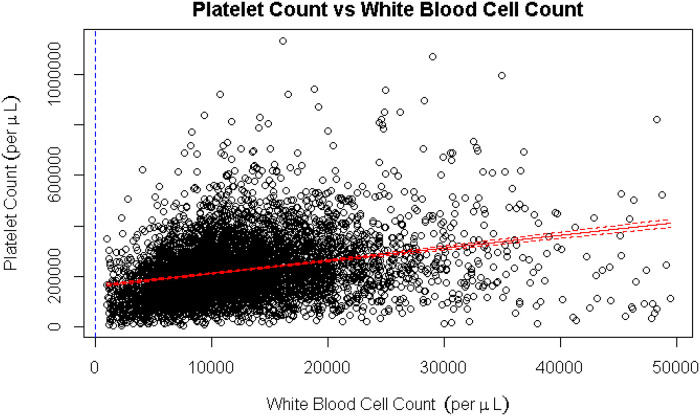
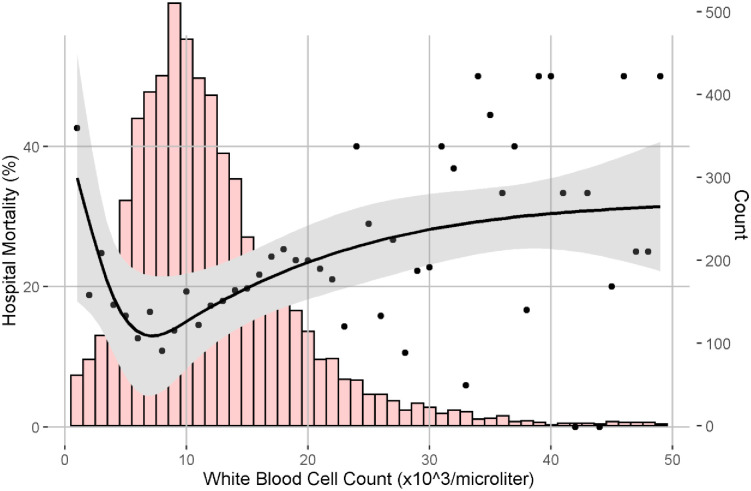
We identified 5,909 ICU patients with suspected infection; 250 (4.2%) had leukopenia. Leukopenia was associated with increased in-hospital mortality compared with leukocytosis (OR, 1.5; 95% CI 1.1-1.9). After adjusting for demographics and comorbidities in the Sepsis-3 consensus model, leukopenia remained associated with increased risk of mortality compared with leukocytosis (OR 1.6, 95% CI 1.2-2.2). Further adjustment for the platelet component of the SOFA attenuated the association between leukopenia and mortality (OR decreased from 1.5 to 1.1). However, 83 (1.4%) of patients had leukopenia without thrombocytopenia and 14 had leukopenia prior to thrombocytopenia.
Among ICU patients with suspected infection, leukopenia was associated with increased risk of death compared with leukocytosis. Due to correlation with thrombocytopenia, leukopenia did not independently improve the prognostic validity of SOFA; however, leukopenia may present as a sign of sepsis prior to thrombocytopenia in a small subset of patients.
虽然白细胞增多和白细胞减少都被认为是全身炎症反应综合征的标准,但白细胞减少通常不被认为是感染的正常反应。我们试图评估白细胞减少作为 Sepsis-3 框架内感染定义性血液器官功能障碍的败血症征象的预后有效性。我们假设白细胞减少与疑似感染患者的白细胞增多相比,与更高的死亡率风险相关。
我们使用医疗信息市场 1.4 版重症监护 III 数据库进行了回顾性队列研究。多变量回归模型用于评估疑似感染患者(由 Sepsis-3 定义)的白细胞减少与死亡率之间的关联。
我们确定了 5909 名 ICU 疑似感染患者;250 名(4.2%)患者存在白细胞减少症。与白细胞增多症相比,白细胞减少症与住院期间死亡率增加相关(比值比,1.5;95%置信区间,1.1-1.9)。在 Sepsis-3 共识模型中调整了人口统计学和合并症后,白细胞减少症与死亡率增加的风险仍相关(比值比 1.6,95%置信区间,1.2-2.2)。进一步调整 SOFA 的血小板成分可减弱白细胞减少症与死亡率之间的关联(比值比从 1.5 降低至 1.1)。然而,83 名(1.4%)患者存在无血小板减少症的白细胞减少症,且 14 名患者在血小板减少症之前存在白细胞减少症。
在 ICU 疑似感染患者中,与白细胞增多症相比,白细胞减少症与死亡风险增加相关。由于与血小板减少症相关,白细胞减少症并未独立提高 SOFA 的预后有效性;然而,在一小部分患者中,白细胞减少症可能先于血小板减少症出现败血症的迹象。