Zirpe Kapil G, Tiwari Anand M, Gurav Sushma K, Deshmukh Abhijit M, Suryawanshi Prasad B, Wankhede Prajkta P, Kapse Upendrakumar S, Bhoyar Abhaya P, Khan Afroz Z, Malhotra Ria V, Kusalkar Pranoti H, Chavan Kaustubh J, Naik Seema A, Bhalke Rahul B, Bhosale Ninad N, Makhija Sonika V, Kuchimanchi Venkata N, Jadhav Amol S, Deshmukh Kedar R, Kulkarni Gaurav S
Department of Neuro Trauma Stroke Unit, Grant Medical Foundation's Ruby Hall Clinic, Pune, Maharashtra, India.
Department of Critical Care, Grant Medical Foundation's Ruby Hall Clinic, Pune, Maharashtra, India.
Indian J Crit Care Med. 2021 May;25(5):493-498. doi: 10.5005/jp-journals-10071-23816.
Severe acute respiratory distress syndrome associated with coronavirus disease-2019 (COVID-19) (CARDS) pneumonitis presents a clinical challenge as regards to the timing of intubation and ambiguity of outcome. There is a lack of clear consensus on when to switch patients from trials of noninvasive therapies to invasive mechanical ventilation. We investigated the effect of the timing of intubation from the time of admission on the clinical outcome of CARDS.
The aim and objective was to analyze the effect of timing of intubation early (within 48 hours of admission to critical care unit) versus delayed (after 48 hours of admission to critical care unit) on mortality in severe CARDS patients.
A retrospective observational study performed in a 28-bedded COVID-19 intensive care unit of a tertiary care hospital in Pune, India. All patients admitted between April 1, 2020, and October 15, 2020, with confirmed COVID-19 (RT-PCR positive) requiring mechanical ventilation were included in the study.
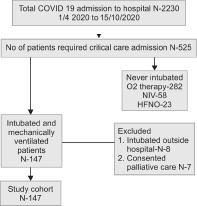
The primary outcome was in-hospital mortality. Among 2,230 patients that were admitted to the hospital, 525 required critical care (23.5%), invasive mechanical ventilation was needed in 162 patients and 147 (28%) of critical care admission were included in the study cohort after exclusion. Seventy-five patients (51%) were intubated within 48 hours of critical care admission (early group) and 72 (48.9%) were intubated after 48 hours of critical care admission (delayed group). With regards to the total of 147 included patients; male patients were 74.1% with a median age of 59 years (interquartile range, 51-68 years). Diabetes (44.9%) and hypertension (43.5%) were the most common comorbidities. Higher admission acute physiology and chronic health evaluation II scores and lower absolute lymphocyte count were observed in patients intubated within 48 hours. The early intubated group had a mortality of 60% whereas the same was observed as 77.7% in delayed intubation group, and this difference was statistically significant ( = 0.02).
Current study concludes that early intubation is associated with improved survival rates in severe CARDS patients.
Zirpe KG, Tiwari AM, Gurav SK, Deshmukh AM, Suryawanshi PB, Wankhede PP, Timing of Invasive Mechanical Ventilation and Mortality among Patients with Severe COVID-19-associated Acute Respiratory Distress Syndrome. Indian J Crit Care Med 2021;25(5):493-498.
与2019冠状病毒病(COVID-19)相关的重症急性呼吸窘迫综合征(CARDS)肺炎在插管时机和预后的不确定性方面带来了临床挑战。对于何时将患者从无创治疗试验转为有创机械通气,目前尚无明确共识。我们研究了从入院时开始的插管时机对CARDS临床结局的影响。
分析早期(重症监护病房入院后48小时内)与延迟(重症监护病房入院后48小时后)插管时机对重症CARDS患者死亡率的影响。
在印度浦那一家三级医院的拥有28张床位的COVID-19重症监护病房进行了一项回顾性观察研究。纳入2020年4月1日至2020年10月15日期间所有确诊为COVID-19(逆转录聚合酶链反应阳性)且需要机械通气的患者。
主要结局为院内死亡率。在2230名入院患者中,525名需要重症监护(23.5%),162名患者需要有创机械通气,排除后147名(28%)重症监护入院患者纳入研究队列。75名患者(51%)在重症监护入院后48小时内插管(早期组),72名(48.9%)在重症监护入院后48小时后插管(延迟组)。对于总共147名纳入患者;男性患者占74.1%,中位年龄为59岁(四分位间距,51 - 68岁)。糖尿病(44.9%)和高血压(43.5%)是最常见的合并症。48小时内插管的患者入院时急性生理与慢性健康状况评分II更高,绝对淋巴细胞计数更低。早期插管组死亡率为60%,而延迟插管组为77.7%,差异具有统计学意义( = 0.02)。
当前研究得出结论,早期插管与重症CARDS患者生存率提高相关。
Zirpe KG, Tiwari AM, Gurav SK, Deshmukh AM, Suryawanshi PB, Wankhede PP, 重症COVID-19相关急性呼吸窘迫综合征患者有创机械通气时机与死亡率。《印度重症监护医学杂志》2021;25(5):493 - 498。