Hyman Jaime B, Leibner Evan S, Tandon Pranai, Egorova Natalia N, Bassily-Marcus Adel, Kohli-Seth Roopa, Arvind Varun, Chang Helena L, Lin Hung-Mo, Levin Matthew A
Department of Anesthesiology, Yale University School of Medicine, New Haven, CT.
Institute for Critical Care Medicine, Icahn School of Medicine at Mount Sinai, New York, NY.
Crit Care Explor. 2020 Oct 21;2(10):e0254. doi: 10.1097/CCE.0000000000000254. eCollection 2020 Oct.
To examine whether increasing time between admission and intubation was associated with mortality in patients with coronavirus disease 2019 who underwent mechanical ventilation.
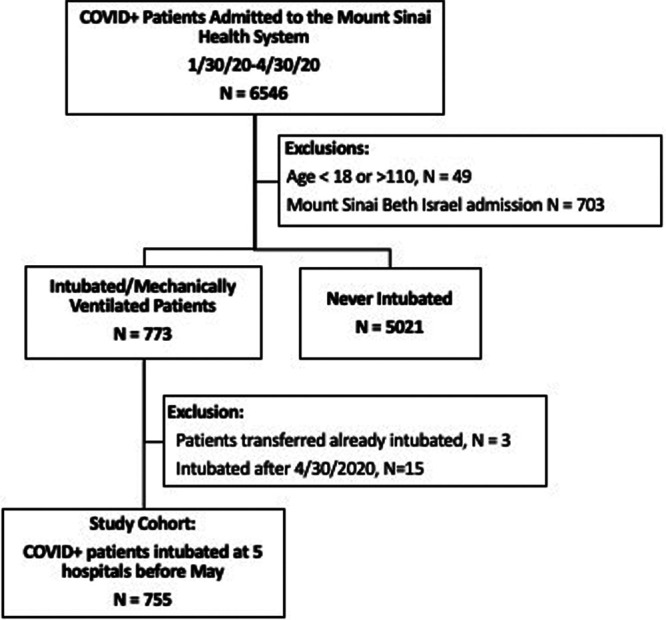
Retrospective cohort study of patients with severe acute respiratory syndrome coronavirus 2 infection who were admitted between January 30, 2020, and April 30, 2020, and underwent intubation and mechanical ventilation prior to May 1, 2020. Patients were followed up through August 15, 2020.
Five hospitals within the Mount Sinai Health System in New York City, NY.
Adult patients with severe acute respiratory syndrome coronavirus 2 infection who underwent intubation and mechanical ventilation.
Tracheal intubation and mechanical ventilation.
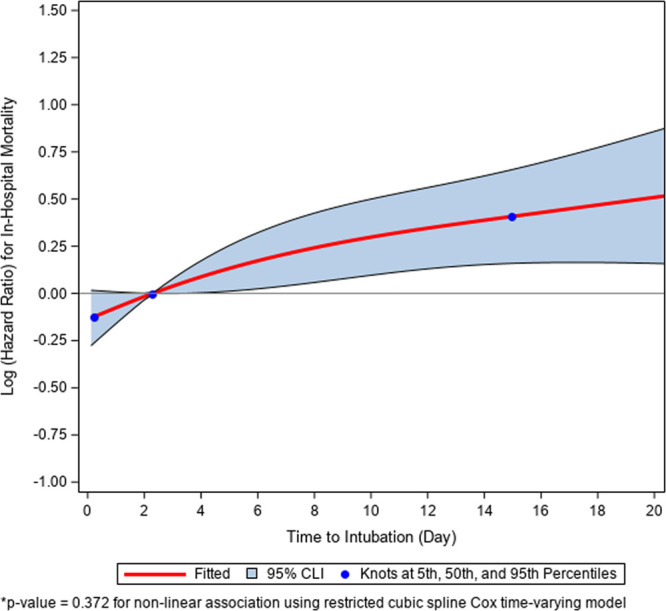
The primary outcome was in-hospital mortality. A hospital-stratified time-varying Cox model was used to evaluate the effect of time from admission to intubation on in-hospital death. A total of 755 adult patients out of 5,843 admitted with confirmed severe acute respiratory syndrome coronavirus 2 infection underwent tracheal intubation and mechanical ventilation during the study period. The median age of patients was 65 years (interquartile range, 56-72 yr) and 64% were male. As of the time of follow-up, 121 patients (16%) who were intubated and mechanically ventilated had been discharged home, 512 (68%) had died, 113 (15%) had been discharged to a skilled nursing facility, and 9 (1%) remained in the hospital. The median time from admission to intubation was 2.3 days (interquartile range, 0.6-6.3 d). Each additional day between hospital admission and intubation was significantly associated with higher in-hospital death (adjusted hazard ratio, 1.03; 95% CI, 1.01-1.05).
Among patients with coronavirus disease 2019 who were intubated and mechanically ventilated, intubation earlier in the course of hospital admission may be associated with improved survival.
探讨2019冠状病毒病患者机械通气时,入院至插管时间延长是否与死亡率相关。
对2020年1月30日至2020年4月30日期间收治的严重急性呼吸综合征冠状病毒2感染患者进行回顾性队列研究,这些患者在2020年5月1日前接受了插管和机械通气。对患者随访至2020年8月15日。
纽约市西奈山医疗系统内的五家医院。
接受插管和机械通气的严重急性呼吸综合征冠状病毒2感染成年患者。
气管插管和机械通气。
主要结局为院内死亡率。采用医院分层时变Cox模型评估入院至插管时间对院内死亡的影响。在研究期间,5843例确诊为严重急性呼吸综合征冠状病毒2感染的入院患者中,共有755例成年患者接受了气管插管和机械通气。患者的中位年龄为65岁(四分位间距,56 - 72岁),64%为男性。截至随访时,121例接受插管和机械通气的患者(16%)已出院回家,512例(68%)死亡,113例(15%)出院至专业护理机构,9例(1%)仍住院。入院至插管的中位时间为2.3天(四分位间距,0.6 - 6.3天)。入院至插管每增加一天,院内死亡风险显著增加(校正风险比,1.03;95%置信区间,1.01 - 1.05)。
在接受插管和机械通气的2019冠状病毒病患者中,入院早期插管可能与生存率提高相关。