Department of Internal Medicine, Unfallkrankenhaus Berlin, Berlin, Germany.
Medical Department, Division of Cardiology and Angiology, Centre for cardiovascular Telemedicine, Charité-Universitätsmedizin Berlin, Charitéplatz 1, Berlin, D-10117, Germany.
ESC Heart Fail. 2021 Oct;8(5):3613-3620. doi: 10.1002/ehf2.13413. Epub 2021 Jun 28.
Telemedical emergency services for heart failure (HF) patients are usually provided during business hours. However, many emergencies occur outside of business hours. This study evaluates if a 24/7 telemedical emergency service is needed for the remote management of high-risk HF patients.
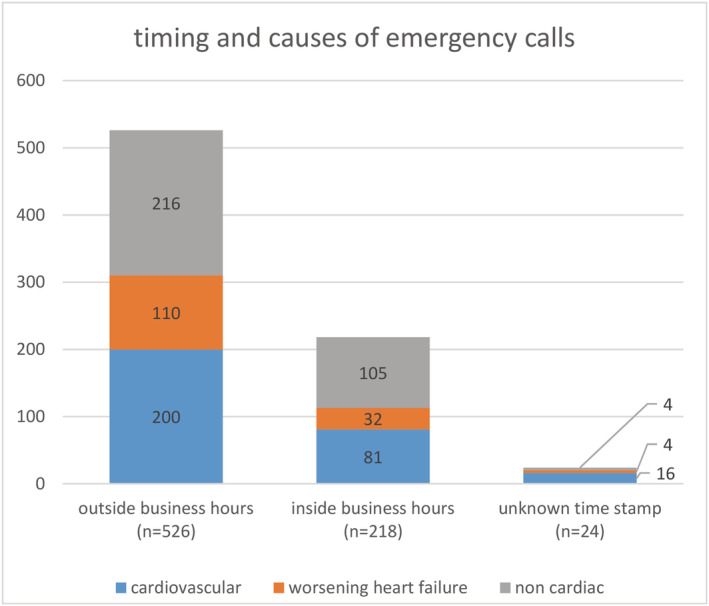
The study included 1119 patients merged from the TIM-HF and TIM-HF2 trials [age 69 ± 11, 73% male, left ventricular ejection fraction 37% ± 13, 557 New York Heart Association (NYHA) II/562 NYHA III]. Patients received a 24/7 physician-guided emergency service provided by the telemedical centre (TMC) in addition to remote management within business hours. During emergency calls, patient status, symptoms, electronic patient record, and instant telemonitoring data were evaluated by the TMC physician. Following diagnosis, patients were referred for hospital admission or instructed to stay at home. Apart from the TMC, patients could place a call to the public emergency service at any time. Seven hundred sixty-eight emergency calls were placed over 1383 patient years (0.56 calls/patient year). Five hundred twenty-six calls (69%) occurred outside business hours. There were 146 (19%) emergency calls for worsening HF, 297 (39%) other cardiovascular, and 325 (42%) non-cardiac causes, with a similar pattern inside and outside business hours. Of the 1119 patients, 417 (37%) placed at least one emergency call. Patients with NYHA Class III, higher N-terminal prohormone of brain natriuretic peptide (>1.400 pg/mL) levels, ischaemic aetiology of HF, implanted defibrillator, and impaired renal function had a higher probability of placing emergency calls. During study follow-up, patients who made an emergency call had a higher all-cause mortality (22% vs. 11%, P = 0.007 in TIM-HF; 16% vs. 4%, P < 0.001 in TIM-HF2) and more unplanned hospitalizations (324 vs. 162, P < 0.001 in TIM-HF; 545 vs. 180, P < 0.001 in TIM-HF2). Of the total 1,211 unplanned hospital admissions, 492 (41%) were initiated by a patient emergency call. Three hundred seventy-nine calls (49%) were placed to the TMC, whereas 389 calls (51%) were made to the public emergency service. Three hundred twenty-six (84%) of the calls to the public emergency service resulted in acute hospitalizations. The TMC initiated 202 (53%) hospital admissions; 177 (47%) patients were advised to stay at home. All patients that remained at home were alive during a prespecified safety period of 7 days post-call. Diagnoses made by the TMC physician were confirmed in 83% of cases by the hospital.
A telemedical emergency service for high-risk HF patients is safe and should operate 24/7 to reduce unplanned hospitalizations. Emergency calls could be considered as a marker for higher morbidity and mortality.
心力衰竭(HF)患者的远程医疗急救服务通常在工作时间内提供。然而,许多紧急情况发生在工作时间之外。本研究评估 24/7 远程医疗急救服务是否对高危 HF 患者的远程管理是必要的。
这项研究纳入了 TIM-HF 和 TIM-HF2 试验合并的 1119 例患者[年龄 69±11,73%为男性,左心室射血分数 37%±13,557 例纽约心功能分级(NYHA)Ⅱ/562 例 NYHA Ⅲ]。患者在接受远程管理的同时,还接受了由远程医疗中心(TMC)提供的 24/7 医生指导的紧急服务。在紧急呼叫期间,TMC 医生会评估患者的状态、症状、电子病历和即时远程监测数据。诊断后,患者被转至医院就诊或告知留在家中。除 TMC 外,患者可在任何时间拨打公共急救服务电话。在 1383 患者年期间(0.56 次/患者年)共拨打了 768 次紧急电话。526 次呼叫(69%)发生在非工作时间。有 146 次(19%)是 HF 恶化的紧急呼叫,297 次(39%)是其他心血管紧急呼叫,325 次(42%)是非心脏紧急呼叫,工作时间内外的情况相似。在 1119 例患者中,417 例(37%)至少拨打了一次紧急电话。NYHA 分级 III、较高的脑钠肽前体(NT-proBNP)水平(>1400pg/ml)、HF 的缺血性病因、植入式除颤器和肾功能受损的患者更有可能拨打紧急电话。在研究随访期间,拨打紧急电话的患者全因死亡率更高(TIM-HF 中为 22% vs. 11%,P=0.007;TIM-HF2 中为 16% vs. 4%,P<0.001),无计划住院治疗也更多(TIM-HF 中为 324 次 vs. 162 次,P<0.001;TIM-HF2 中为 545 次 vs. 180 次,P<0.001)。在总共 1211 例非计划性住院治疗中,有 492 例(41%)是由患者紧急电话引发的。379 次电话(49%)是拨打给 TMC 的,而 389 次电话(51%)是拨打给公共急救服务的。拨打公共急救服务的 326 次电话(84%)导致了急性住院治疗。TMC 发起了 202 次(53%)住院治疗;177 名(47%)患者被建议留在家中。所有在家中的患者在电话后 7 天的预定安全期内均存活。TMC 医生做出的诊断在医院得到了 83%的确认。
高危 HF 患者的远程医疗急救服务是安全的,应 24/7 运行以减少非计划性住院治疗。紧急电话可被视为更高发病率和死亡率的标志。