Naik Marcel G, Budde Klemens, Koehler Kerstin, Vettorazzi Eik, Pigorsch Mareen, Arkossy Otto, Stuard Stefano, Duettmann Wiebke, Koehler Friedrich, Winkler Sebastian
Charité-Universitätsmedizin Berlin, Department of Nephrology and Medical Intensive Care, Charité University Medicine Berlin, Berlin, Germany.
Berlin Institute of Health, Charité Medical University of Berlin, Berlin, Germany.
Front Med (Lausanne). 2022 Jul 11;9:917466. doi: 10.3389/fmed.2022.917466. eCollection 2022.
Remote patient management (RPM) in heart failure (HF) patients has been investigated in several prospective randomized trials. The Telemedical Interventional Management in Heart Failure II (TIM-HF2)-trial showed reduced all-cause mortality and hospitalizations in heart failure (HF) patients using remote patient management (RPM) vs. usual care (UC). We report the trial's results for prespecified eGFR-subgroups.
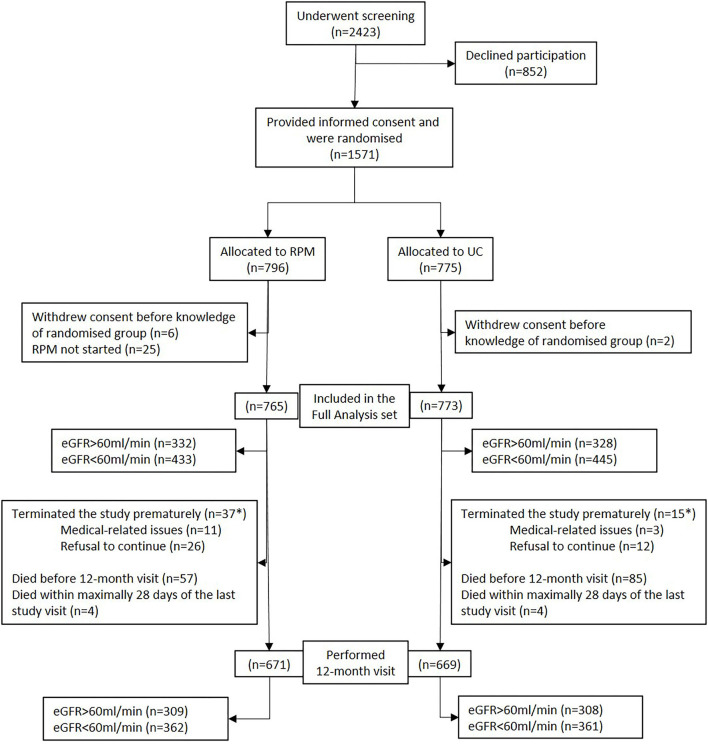
TIM-HF2 was a prospective, randomized, controlled, parallel-group, unmasked (with randomization concealment), multicenter trial. A total of 1,538 patients with stable HF were enrolled in Germany from 2013 to 2017 and randomized to RPM (+UC) or UC. Using CKD-EPI-formula at baseline, prespecified subgroups were defined. In RPM, patients transmitted their vital parameters daily. The telemedical center reviewed and co-operated with the patient's General Practitioner (GP) and cardiologist. In UC, patients were treated by their GPs or cardiologist applying the current guidelines for HF management and treatment. The primary endpoint was the percentage of days lost due to unplanned cardiovascular hospitalizations or death, secondary outcomes included hospitalizations, all-cause, and cardiovascular mortality.
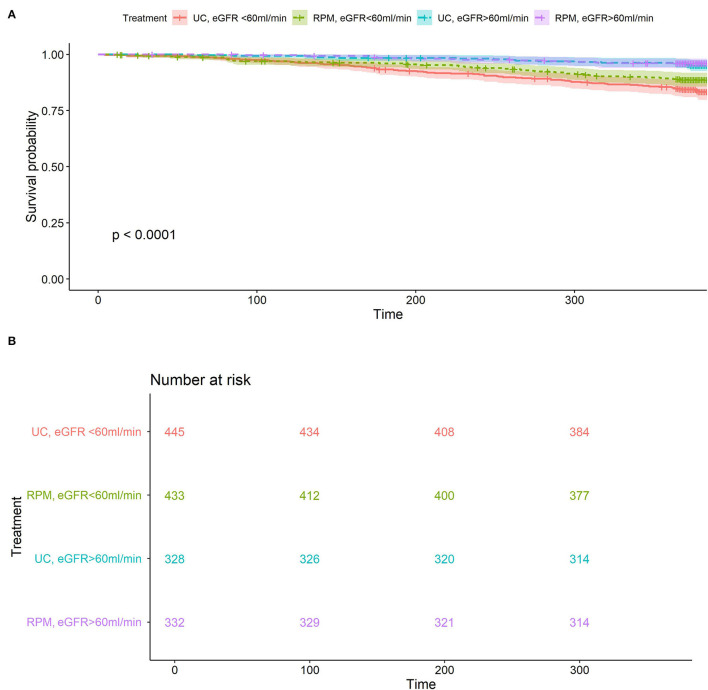
Our sub analysis showed no difference between RPM and UC in both eGFR-subgroups for the primary endpoint (<60 ml/min/1.73 m: 40.9% vs. 43.6%, = 0.1, ≥60 ml/min/1.73 m 26.5 vs. 29.3%, = 0.36). In patients with eGFR < 60 ml/min/1.73 m, 1-year-survival was higher in RPM than UC (89.4 vs. 84.6%, = 0.02) with an incident rate ratio (IRR) 0.67 ( = 0.03). In the recurrent event analysis, HF hospitalizations and all-cause death were lower in RPM than UC in both eGFR-subgroups (<60 ml/min/1.73 m: IRR 0.70, = 0.02; ≥60 ml/min/1.73 m: IRR 0.64, = 0.04). In a cox regression analysis, age, NT-pro BNP, eGFR, and BMI were associated with all-cause mortality.
RPM may reduce all-cause mortality and HF hospitalizations in patients with HF and eGFR < 60 ml/min/1.73 m. HF hospitalizations and all-cause death were lower in RPM in both eGFR-subgroups in the recurrent event analysis. Further studies are needed to investigate and confirm this finding.
在多项前瞻性随机试验中对心力衰竭(HF)患者的远程患者管理(RPM)进行了研究。心力衰竭远程医疗干预管理II(TIM-HF2)试验表明,与常规治疗(UC)相比,使用远程患者管理(RPM)的心力衰竭(HF)患者全因死亡率和住院率降低。我们报告了针对预先指定的估算肾小球滤过率(eGFR)亚组的试验结果。
TIM-HF2是一项前瞻性、随机、对照、平行组、非盲法(有随机化隐藏)的多中心试验。2013年至2017年在德国共招募了1538例稳定HF患者,并随机分为RPM(+UC)组或UC组。根据基线时的CKD-EPI公式定义预先指定的亚组。在RPM组中,患者每天传输其生命体征参数。远程医疗中心与患者的全科医生(GP)和心脏病专家进行审查和合作。在UC组中,患者由其GP或心脏病专家按照当前HF管理和治疗指南进行治疗。主要终点是因计划外心血管住院或死亡而损失的天数百分比,次要结局包括住院、全因死亡率和心血管死亡率。
我们的亚组分析显示,在两个eGFR亚组中,RPM组和UC组在主要终点方面无差异(eGFR<60 ml/min/1.73 m²:40.9%对43.6%,P = 0.1;eGFR≥60 ml/min/1.73 m²:26.5%对29.3%,P = 0.36)。在eGFR<60 ml/min/1.73 m的患者中,RPM组的1年生存率高于UC组(89.4%对84.6%,P = 0.02),发生率比(IRR)为0.67(P = 0.03)。在复发事件分析中,在两个eGFR亚组中,RPM组的HF住院率和全因死亡率均低于UC组(eGFR<60 ml/min/1.73 m²:IRR 0.70,P = 0.02;eGFR≥60 ml/min/1.73 m²:IRR 0.64,P = 0.04)。在cox回归分析中,年龄、N末端脑钠肽前体(NT-pro BNP)、eGFR和体重指数(BMI)与全因死亡率相关。
RPM可能降低HF且eGFR<60 ml/min/1.73 m患者中的全因死亡率和HF住院率。在复发事件分析中,两个eGFR亚组中RPM组的HF住院率和全因死亡率均较低。需要进一步研究来调查和证实这一发现。