Department of Emergency Medicine, College of Medicine, Korea University, Seoul, Korea.
Department of Preventive Medicine, College of Medicine, Korea University Hospital, Seoul, Korea.
J Korean Med Sci. 2021 Jun 28;36(25):e173. doi: 10.3346/jkms.2021.36.e173.
Survival and post-cardiac arrest care vary considerably by hospital, region, and country. In the current study, we aimed to analyze mortality in patients who underwent cardiac arrest by hospital level, and to reveal differences in patient characteristics and hospital factors, including post-cardiac arrest care, hospital costs, and adherence to changes in resuscitation guidelines.
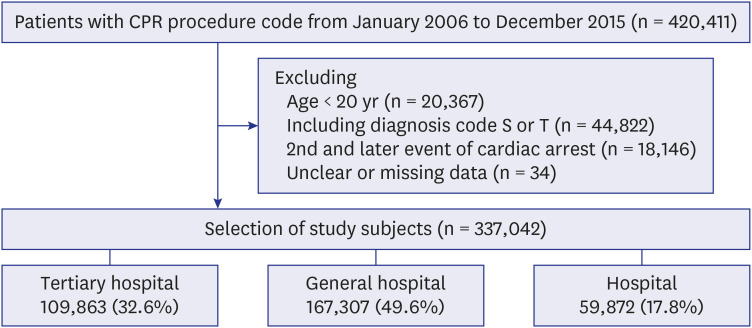
We enrolled adult patients (≥ 20 years) who suffered non-traumatic cardiac arrest from 2006 to 2015. Patient demographics, insurance type, admission route, comorbidities, treatments, and hospital costs were extracted from the National Health Insurance Service database. We categorized patients into tertiary hospital, general hospital, and hospital groups according to the level of the hospital where they were treated. We analyzed the patients' characteristics, hospital factors, and mortalities among the three groups. We also analyzed post-cardiac arrest care before and after the 2010 guideline changes. The primary end-point was 30 days and 1 year mortality rates.
The tertiary hospital, general hospital, and hospital groups represented 32.6%, 49.6%, and 17.8% of 337,042 patients, respectively. The tertiary and general hospital groups were younger, had a lower proportion of medical aid coverage, and fewer comorbidities, compared to the hospital group. Post-cardiac arrest care, such as percutaneous coronary intervention, targeted temperature management, and extracorporeal membrane oxygenation, were provided more frequently in the tertiary and general hospital groups. After adjusting for age, sex, insurance type, urbanization level, admission route, comorbidities, defibrillation, resuscitation medications, angiography, and guideline changes, the tertiary and general hospital groups showed lower 1-year mortality (tertiary hospital vs. general hospital vs. hospital, adjusted odds ratios, 0.538 vs. 0.604 vs. 1; < 0.001). After 2010 guideline changes, a marked decline in atropine use and an increase in post-cardiac arrest care were observed in the tertiary and general hospital groups.
The tertiary and general hospital groups showed lower 30 days and 1 year mortality rates than the hospital group, after adjusting for patient characteristics and hospital factors. Higher-level hospitals provided more post-cardiac arrest care, which led to high hospital costs, and showed good adherence to the guideline change after 2010.
存活率和心脏骤停后护理在医院、地区和国家之间存在很大差异。在本研究中,我们旨在分析按医院级别进行的心脏骤停患者的死亡率,并揭示患者特征和医院因素的差异,包括心脏骤停后护理、医院费用以及对复苏指南变化的遵循情况。
我们纳入了 2006 年至 2015 年期间患有非创伤性心脏骤停的成年患者(≥20 岁)。从国民健康保险服务数据库中提取患者人口统计学、保险类型、入院途径、合并症、治疗方法和医院费用等信息。我们根据患者治疗的医院级别,将患者分为三级医院、综合医院和医院组。我们分析了三组患者的特征、医院因素和死亡率。我们还分析了 2010 年指南变化前后的心脏骤停后护理情况。主要终点为 30 天和 1 年的死亡率。
三级医院、综合医院和医院组分别占 337042 例患者的 32.6%、49.6%和 17.8%。与医院组相比,三级和综合医院组更年轻,医疗保险覆盖率更低,合并症更少。心脏骤停后护理,如经皮冠状动脉介入治疗、目标温度管理和体外膜肺氧合,在三级和综合医院组中更频繁地实施。在调整年龄、性别、保险类型、城市化水平、入院途径、合并症、除颤、复苏药物、血管造影和指南变化后,三级和综合医院组的 1 年死亡率较低(三级医院 vs. 综合医院 vs. 医院,调整后的优势比分别为 0.538 vs. 0.604 vs. 1;<0.001)。2010 年指南变化后,在三级和综合医院组中,阿托品的使用明显减少,心脏骤停后护理增加。
在调整患者特征和医院因素后,与医院组相比,三级和综合医院组的 30 天和 1 年死亡率较低。高水平医院提供了更多的心脏骤停后护理,导致了高昂的医院费用,并在 2010 年后对指南变化有较好的遵循。