Sagara Issaka, Woodford John, Kone Mamady, Assadou Mahamadoun Hamady, Katile Abdoulaye, Attaher Oumar, Zeguime Amatigue, Doucoure M'Bouye, Higbee Emily, Lane Jacquelyn, Mohan Rathy, Doritchamou Justin, Zaidi Irfan, Esposito Dominic, Kwan Jennifer, Sadtler Kaitlyn, Dicko Alassane, Duffy Patrick E
Malaria Research and Training Center/University of Sciences, Techniques and Techniques of Bamako, Bamako, Mali.
Laboratory of Malaria Immunology and Vaccinology, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Maryland, Bethesda, USA.
Clin Infect Dis. 2022 Mar 23;74(6):1030-1038. doi: 10.1093/cid/ciab589.
The extent of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) exposure and transmission in Mali and the surrounding region is not well understood. We aimed to estimate the cumulative incidence of SARS-CoV-2 in 3 communities and understand factors associated with infection.
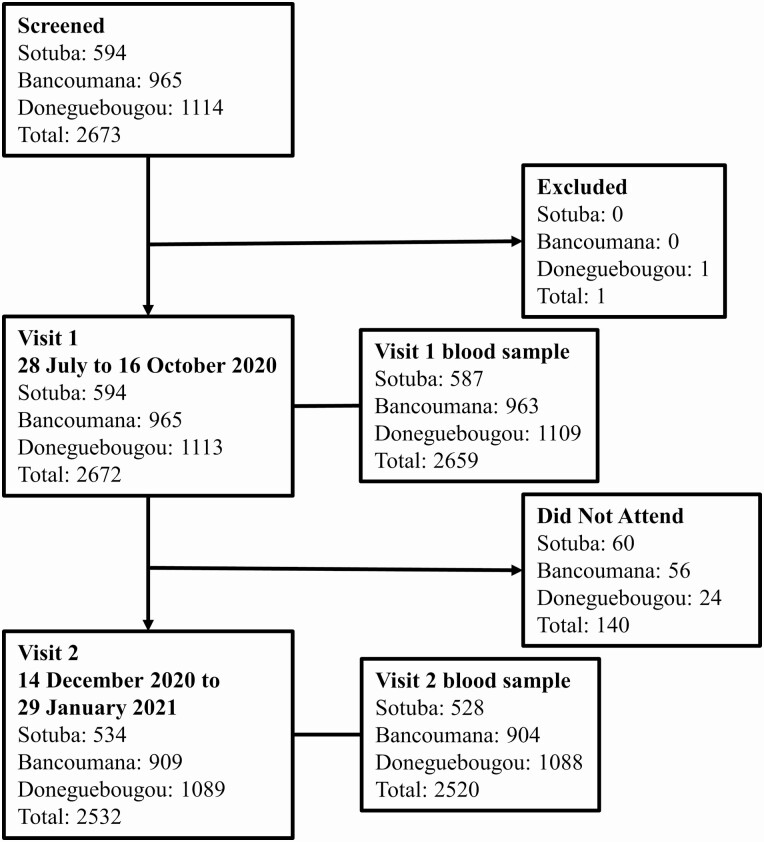
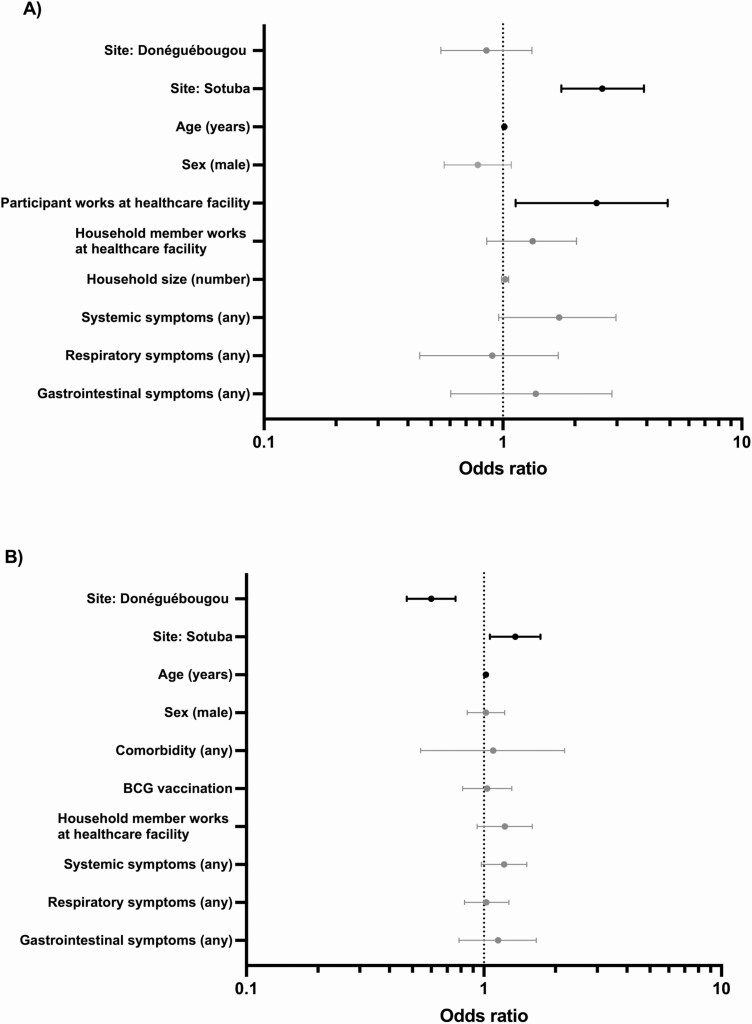
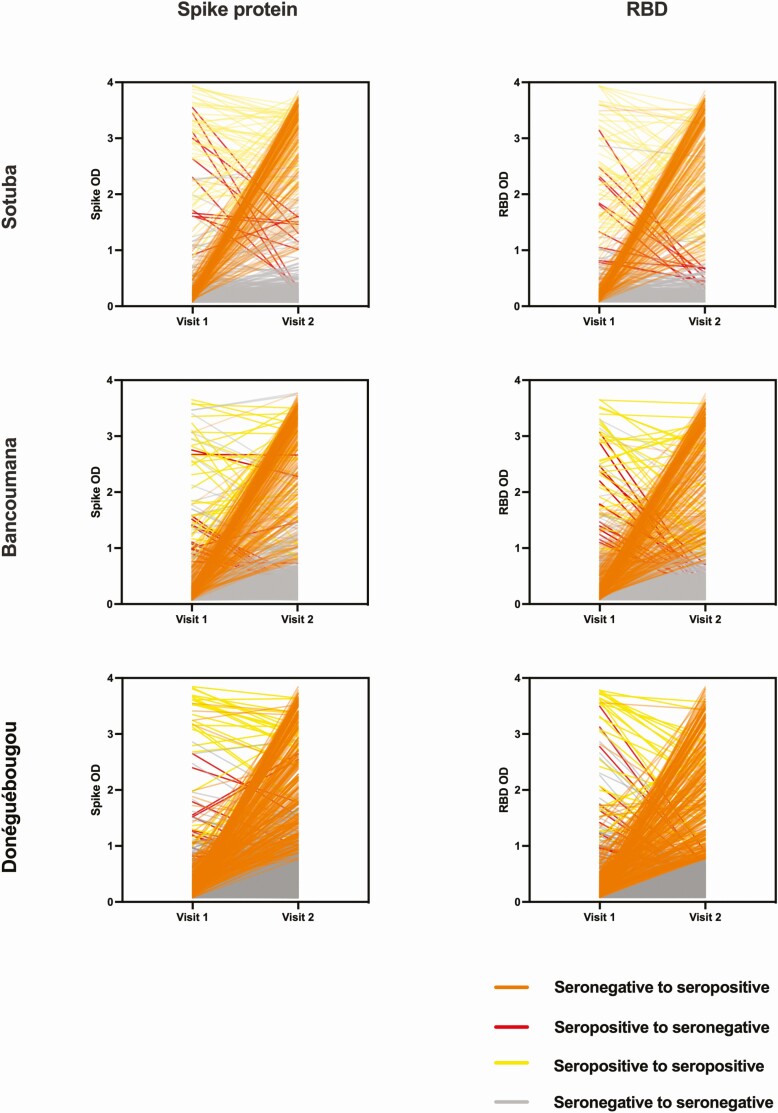
Between July 2020 and January 2021, we collected blood samples and demographic, social, medical, and self-reported symptoms information from residents aged 6 months and older over 2 study visits. SARS-CoV-2 antibodies were measured using a highly specific 2-antigen enzyme-linked immunosorbent assay optimized for use in Mali. We calculated cumulative adjusted seroprevalence for each community and evaluated factors associated with serostatus at each visit by univariate and multivariate analysis.
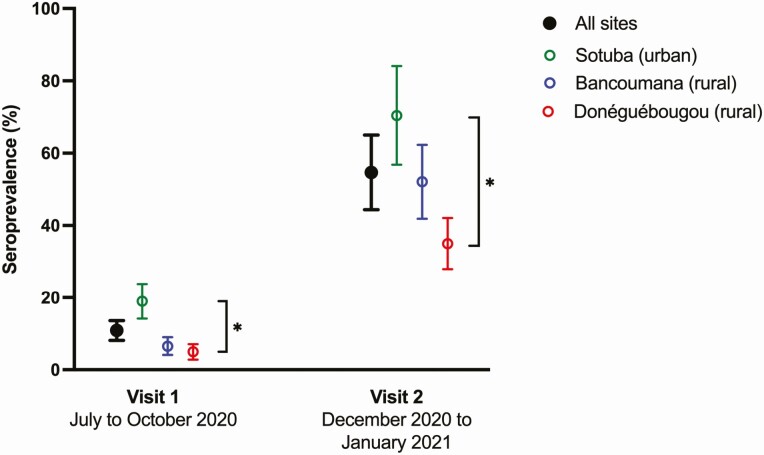
Overall, 94.8% (2533/2672) of participants completed both study visits. A total of 31.3% (837/2672) were aged <10 years, 27.6% (737/2672) were aged 10-17 years, and 41.1% (1098/2572) were aged ≥18 years. The cumulative SARS-CoV-2 exposure rate was 58.5% (95% confidence interval, 47.5-69.4). This varied between sites and was 73.4% in the urban community of Sotuba, 53.2% in the rural town of Bancoumana, and 37.1% in the rural village of Donéguébougou. Study site and increased age were associated with serostatus at both study visits. There was minimal difference in reported symptoms based on serostatus.
The true extent of SARS-CoV-2 exposure in Mali is greater than previously reported and may now approach hypothetical "herd immunity" in urban areas. The epidemiology of the pandemic in the region may be primarily subclinical and within background illness rates.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)在马里及周边地区的暴露和传播程度尚不清楚。我们旨在估计三个社区中SARS-CoV-2的累积发病率,并了解与感染相关的因素。
在2020年7月至2021年1月期间,我们通过两次研究访视,收集了6个月及以上居民的血液样本以及人口统计学、社会、医疗和自我报告症状信息。使用针对马里优化的高特异性双抗原酶联免疫吸附测定法检测SARS-CoV-2抗体。我们计算了每个社区的累积校正血清阳性率,并通过单因素和多因素分析评估每次访视时与血清状态相关的因素。
总体而言,94.8%(2533/2672)的参与者完成了两次研究访视。共有31.3%(837/2672)的参与者年龄<10岁,27.6%(737/2672)的参与者年龄在10 - 17岁之间,41.1%(1098/2572)的参与者年龄≥18岁。SARS-CoV-2的累积暴露率为58.5%(95%置信区间,47.5 - 69.4)。这在不同地点有所差异,在索图巴城市社区为73.4%,在班库马纳农村镇为53.2%,在多内盖布古农村村为37.1%。研究地点和年龄增长与两次研究访视时的血清状态均相关。基于血清状态的报告症状差异极小。
马里SARS-CoV-2暴露的实际程度高于先前报告的水平,在城市地区可能已接近假设的“群体免疫”。该地区大流行的流行病学特征可能主要为亚临床感染,且处于背景疾病率范围内。