Department of Cardiothoracic Surgery.
Department of Pathology, the Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China.
Medicine (Baltimore). 2021 Jul 2;100(26):e26449. doi: 10.1097/MD.0000000000026449.
Anaplastic lymphoma kinase (ALK) inhibitors have been approved for patients with ALK-rearrangement lung cancer. The effect is superior to the standard first-line therapy of pemetrexed plus platinum-based chemotherapy. However, ALK inhibitors are associated with rare and sometimes fatal adverse events. Organizing pneumonitis (OP) is a rare and serious adverse event usually caused by ceritinib, and it is easily misdiagnosed as infectious pneumonia, metastasis, or cancer progression.
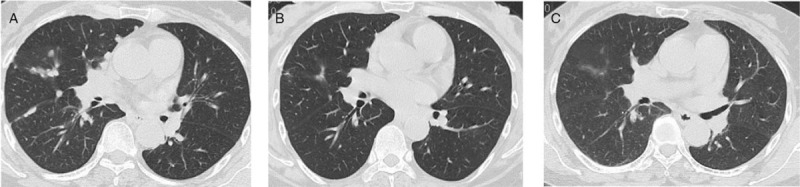
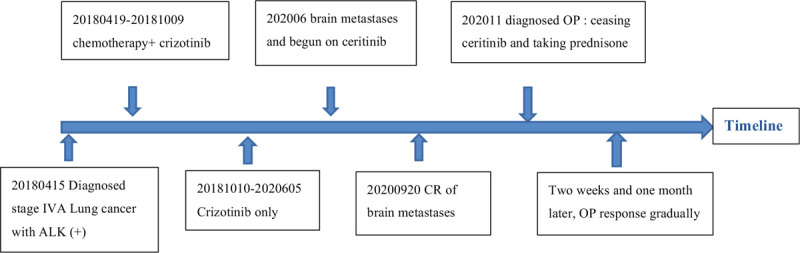
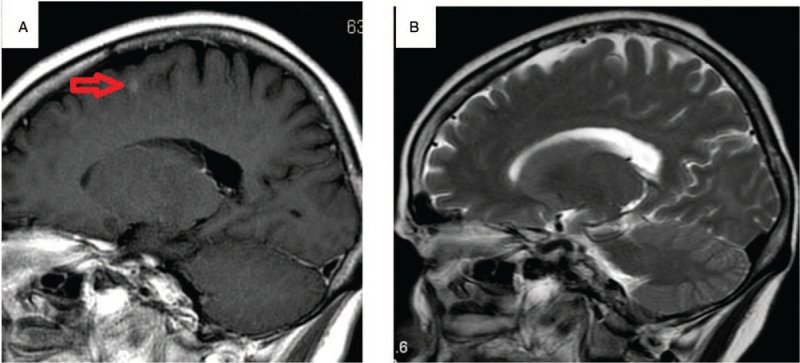
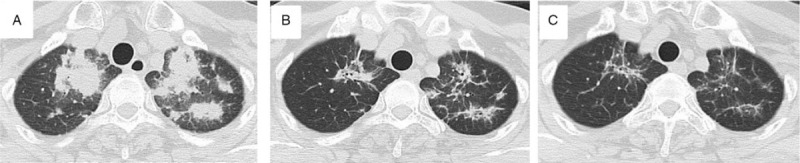
A 56-year-old female presented with chest tightness and dyspnea for more than 10 days. She was previously healthy with no significant medical history. Workup including chest computed tomography (CT), pathological examination of a biopsy specimen, and next-generation sequencing was consistent with a diagnosis of IVA ALK-rearrangement lung adenocarcinoma. She was treated with pemetrexed plus platinum-based chemotherapy and crizotinib concurrently, followed by maintenance therapy with crizotinib alone and she had an almost complete response. However, about 26 months after beginning treatment she developed multiple brain metastases. Crizotinib was discontinued and she was begun on ceritinib. After about 3 months the brain metastases had almost complete response. After 5 months of ceritinib, however, multiple patchy lesions appeared in the bilateral upper lungs.
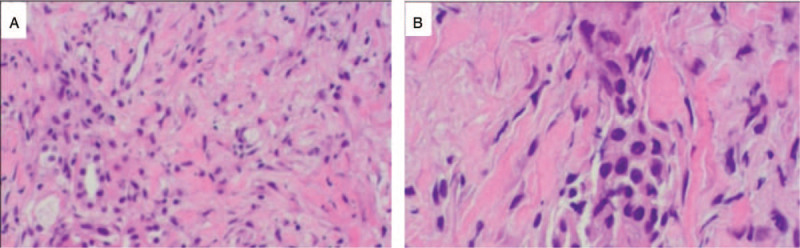
Treatment with antibiotics had no effect and blood and sputum cultures are negative. A CT-guided biopsy of the upper lung was performed, and pathological hematoxylin-eosin staining and immunohistochemical studies were consistent with OP.
Ceritinib was discontinued, she was begun on prednisone 0.5 mg/kg orally every day, and regular follow-up is necessary.
CT of the chest 2 and 4 weeks after beginning prednisone showed the lung lesions to be gradually resolving, and she was continued on prednisone for 2 months and gradually reduced the dose of prednisone every 2 weeks. No related adverse events were occurred in patient.
OP must be differentiated from infectious pneumonia, metastasis, or cancer progression. The mechanism of OP is still unknown and needs further research. Biopsy plays a role in making a diagnosis of OP. In our patient, discontinuing ceritinib and treating her with prednisone resulted in a good outcome.
间变性淋巴瘤激酶(ALK)抑制剂已被批准用于治疗具有 ALK 重排的肺癌患者。其疗效优于培美曲塞联合铂类化疗的标准一线治疗。然而,ALK 抑制剂与罕见且有时致命的不良事件相关。机化性肺炎(OP)是一种罕见且严重的不良事件,通常由塞瑞替尼引起,容易误诊为感染性肺炎、转移或癌症进展。
一名 56 岁女性因胸闷和呼吸困难超过 10 天就诊。她以前身体健康,无重大病史。包括胸部计算机断层扫描(CT)、活检标本的病理检查和下一代测序在内的检查结果均符合 IVA 期 ALK 重排肺腺癌的诊断。她接受了培美曲塞联合铂类化疗和克唑替尼联合治疗,随后单独用克唑替尼维持治疗,几乎完全缓解。然而,大约在开始治疗后 26 个月,她出现了多发性脑转移。停用克唑替尼,开始服用塞瑞替尼。大约 3 个月后,脑转移几乎完全缓解。然而,服用塞瑞替尼 5 个月后,双肺上叶出现多个斑片状病变。
抗生素治疗无效,血和痰培养均为阴性。对肺部进行 CT 引导下活检,行病理苏木精-伊红染色和免疫组织化学研究,结果与 OP 一致。
停用塞瑞替尼,开始口服泼尼松 0.5mg/kg/天,需定期随访。
开始服用泼尼松后 2 和 4 周行胸部 CT 显示肺部病变逐渐缓解,继续服用泼尼松 2 个月,每 2 周逐渐减少泼尼松剂量。患者未发生与治疗相关的不良事件。
OP 必须与感染性肺炎、转移或癌症进展相区别。OP 的发病机制尚不清楚,需要进一步研究。活检在 OP 的诊断中发挥作用。在我们的患者中,停用塞瑞替尼并用泼尼松治疗取得了良好的效果。