Faculty of Medicine and Health, Sydney School of Public Health, The University of Sydney, Camperdown, NSW 2006, Australia.
Maternal and Child Health Division, International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Dhaka 1212, Bangladesh.
Int J Environ Res Public Health. 2021 Jun 2;18(11):5976. doi: 10.3390/ijerph18115976.
Timely initiation of breastfeeding is the first step towards achieving recommended breastfeeding behaviours. Delayed breastfeeding initiation harms neonatal health and survival, including infection associated neonatal mortality. Eighty percent of neonatal deaths occur in the low-and middle-income countries (LMICs), where delayed breastfeeding initiation is the highest. Place and mode of childbirth are important factors determining the time of initiation of breastfeeding. In this study, we report the prevalence of delayed breastfeeding initiation from 58 LMICs and investigate the relationship between place and mode of childbirth and delayed breastfeeding initiation in each country.
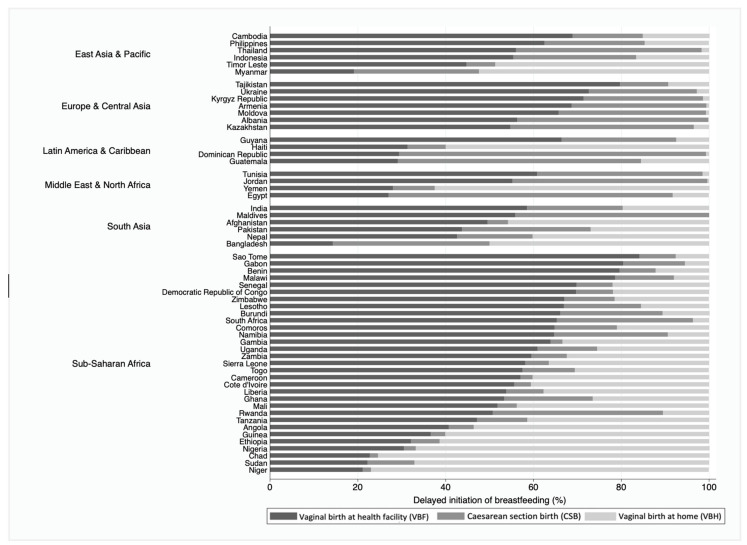
We analysed data from the most recent Demographic and Health Survey (DHS) and Multiple Indicator Cluster Survey (MICS) collected between 2012 and 2017 and reported by 2019. The study sample comprised all women who had a live birth in the 24 months preceding the survey. 'Delayed' initiation of breastfeeding was defined using WHO recommendations as starting breastfeeding after one hour of birth. We coded the stratifying variable for the place and mode of childbirth as "vaginal birth at a facility (VBF)", "caesarean section birth (CSB) ", and "vaginal birth at home (VBH)". We used respondent-level sampling weights to account for individual surveys and de-normalised the standard survey weights to ensure the appropriate contribution of data from each country. We report the prevalence and population attributable fractions with robust standard errors. The population attributable risk identifies the proportion of delayed initiation that we could avert among VBH and CSB if everyone had the same risk of delaying breastfeeding as in VBF.
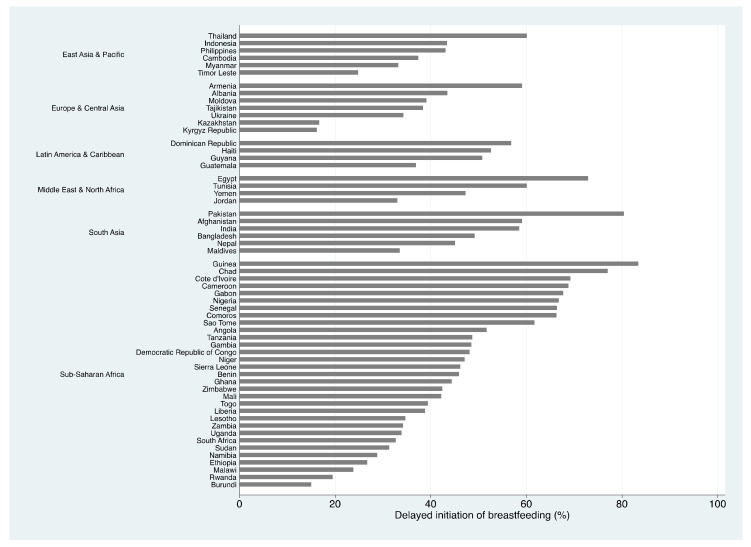
The overall prevalence of delayed initiation of breastfeeding was 53.8% (95% CI 53.3, 54.3), ranging from 15.0% (95% CI 13.8, 16.2) in Burundi to 83.4% (95% CI 80.6, 86.0) in Guinea. The prevalence of delayed initiation of breastfeeding was consistently high among women who experienced caesarean section births; however, there was no direct association with each country's national caesarean section rates. The prevalence of delayed initiation among women who experienced VBF was high in Sub-Saharan Africa and South Asia, even though the CSB rates were low. In some countries, women who give birth vaginally in health facilities were more likely to delay breastfeeding initiation than women who did not. In many places, women who give birth by caesarean section were less likely to delay breastfeeding initiation. Population attributable risk percent for VBH ranged from -28.5% in Ukraine to 22.9% in Moldova, and for CSB, from 10.3% in Guinea to 54.8% in Burundi. On average, across all 58 countries, 24.4% of delayed initiation could be prevented if all women had the same risk of delaying breastfeeding initiation as in VBF.
In general, women who give birth in a health facility were less likely to experience delayed initiation of breastfeeding. Programs could avert much of the delayed breastfeeding initiation in LMICs if the prevalence of delayed initiation amongst women who experience CSB were the same as amongst women who experience VBF. Crucial reforms of health facilities are required to ensure early breastfeeding practices and to create pro-breastfeeding supportive environments as recommended in intervention packages like the Baby-friendly hospital initiative and Early essential newborn care. The findings from this study will guide program managers to identify countries at varying levels of preparedness to establish and maintain a breastfeeding-friendly environment at health facilities. Thus, governments should prioritise intervention strategies to improve coverage and settings surrounding early initiation of breastfeeding while considering the complex role of place and mode of childbirth.
及时开始母乳喂养是实现推荐母乳喂养行为的第一步。延迟开始母乳喂养会损害新生儿的健康和生存,包括与感染相关的新生儿死亡。80%的新生儿死亡发生在中低收入国家(LMICs),而这些国家的延迟母乳喂养发生率最高。分娩地点和方式是决定母乳喂养开始时间的重要因素。在这项研究中,我们报告了来自 58 个 LMICs 的延迟母乳喂养发生率,并调查了每个国家分娩地点和方式与延迟母乳喂养开始之间的关系。
我们分析了 2012 年至 2017 年期间收集并由 2019 年报告的最新人口与健康调查(DHS)和多指标类集调查(MICS)的数据。研究样本包括在调查前 24 个月内有活产的所有妇女。“延迟”开始母乳喂养的定义是根据世界卫生组织的建议,即出生后 1 小时开始母乳喂养。我们将分娩地点和方式的分层变量编码为“设施内阴道分娩(VBF)”、“剖宫产(CSB)”和“家庭内阴道分娩(VBH)”。我们使用受访者层面的抽样权重来考虑每个调查,并对标准调查权重进行去标准化,以确保每个国家的数据都有适当的贡献。我们报告了流行率和人群归因分数,以及稳健的标准误差。人群归因风险识别了如果每个人都像 VBF 一样延迟母乳喂养的风险,我们可以在 VBH 和 CSB 中避免的延迟启动比例。
总体而言,延迟开始母乳喂养的流行率为 53.8%(95%CI 53.3,54.3),范围从布隆迪的 15.0%(95%CI 13.8,16.2)到几内亚的 83.4%(95%CI 80.6,86.0)。经历剖宫产的妇女中,延迟开始母乳喂养的流行率始终很高;然而,这与每个国家的全国剖宫产率没有直接关系。在撒哈拉以南非洲和南亚,即使剖宫产率较低,经历 VBF 的妇女中延迟开始母乳喂养的流行率也很高。在一些国家,在卫生设施中阴道分娩的妇女比没有这样做的妇女更有可能延迟开始母乳喂养。在许多地方,剖宫产的妇女不太可能延迟开始母乳喂养。VBH 的人群归因风险百分比范围从乌克兰的-28.5%到摩尔多瓦的 22.9%,CSB 的人群归因风险百分比范围从几内亚的 10.3%到布隆迪的 54.8%。平均而言,在所有 58 个国家中,如果所有妇女都像 VBF 那样有延迟母乳喂养的风险,那么 24.4%的延迟开始可以预防。
一般来说,在卫生机构分娩的妇女不太可能延迟开始母乳喂养。如果 CSB 经历的妇女中延迟母乳喂养的流行率与 VBF 经历的妇女相同,那么方案可以避免中低收入国家中许多延迟母乳喂养的发生。需要对卫生机构进行重大改革,以确保按照婴儿友好医院倡议和早期基本新生儿护理等干预措施包推荐的那样,实行早期母乳喂养做法,并创造支持母乳喂养的环境。本研究的结果将指导方案管理人员确定各国在建立和维持母乳喂养友好环境方面的准备程度。因此,政府应优先考虑干预策略,以提高早期母乳喂养的覆盖率和环境,同时考虑分娩地点和方式的复杂作用。