Rim Chai Hong, Park Sunmin, Shin In-Soo, Yoon Won Sup
Department of Radiation Oncology, Ansan Hospital, Korea University Medical College, Ansan 15355, Korea.
Graduate School of Education, Dongguk University, Seoul 04620, Korea.
Cancers (Basel). 2021 Jun 10;13(12):2912. doi: 10.3390/cancers13122912.
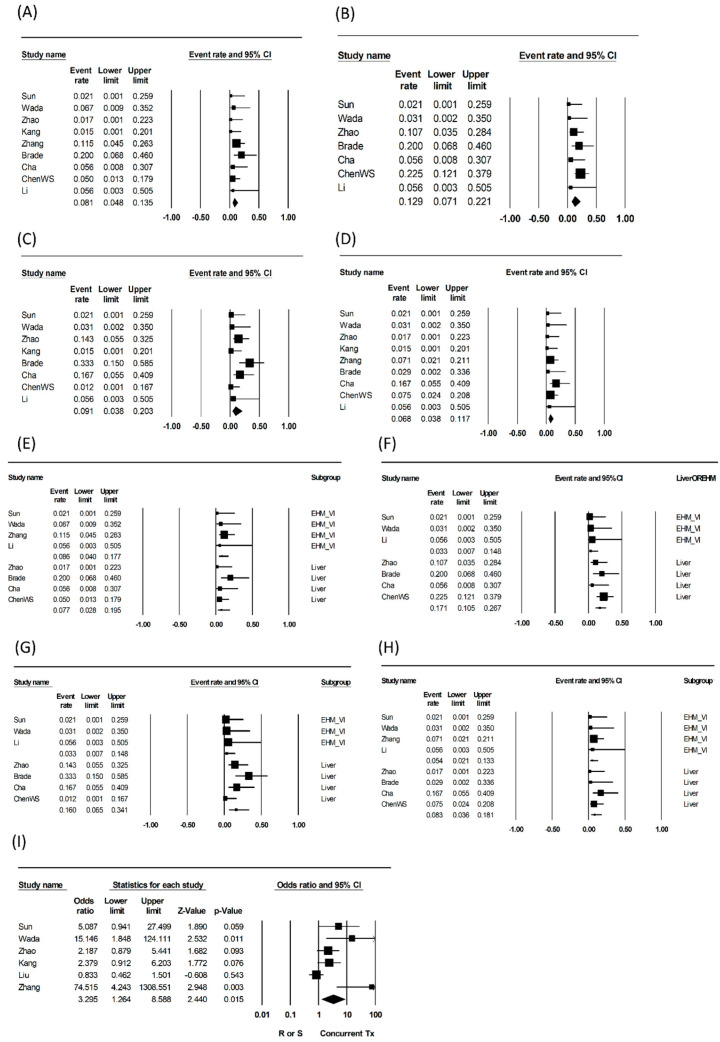
We evaluate the feasibility of a concurrent application of sorafenib and external beam radiation therapy (EBRT) for advanced hepatocellular carcinoma (HCC). PubMed, Embase, Medline, and Cochrane Library were searched up to 9 April 2021. The primary endpoint was grade ≥3 complications, and the secondary endpoint was overall survival (OS). Subgroup analyses were performed for studies with the EBRT targets, intrahepatic vs. non-intrahepatic lesions (e.g., extrahepatic metastases or malignant vessel involvement only). Eleven studies involving 512 patients were included in this meta-analysis. Pooled rates of gastrointestinal, hepatologic, hematologic, and dermatologic grade ≥3 toxicities were 8.1% (95% confidence interval (CI): 4.8-13.5, I = ~0%), 12.9% (95% CI: 7.1-22.1, I = 22.4%), 9.1% (95% CI: 3.8-20.3, I = 51.3%), and 6.8% (95% CI: 3.8-11.7, I = ~0%), respectively. Pooled grade ≥3 hepatologic and hematologic toxicity rates were lower in studies targeting non-intrahepatic lesions than those targeting intrahepatic lesions (hepatologic: 3.3% vs. 17.1%, 0.041; hematologic: 3.3% vs. 16.0%, 0.078). Gastrointestinal and dermatologic grade ≥3 complications were not significantly different between the subgroups. Regarding OS, concurrent treatment was more beneficial than non-concurrent treatment (odds ratio: 3.3, 95% CI: 1.3-8.59, 0.015). One study reported a case of lethal toxicity due to tumor rupture and gastrointestinal bleeding. Concurrent treatment can be considered and applied to target metastatic lesions or local vessel involvement. Intrahepatic lesions should be treated cautiously by considering the target size and hepatic reserve.
我们评估了索拉非尼与外照射放疗(EBRT)联合应用于晚期肝细胞癌(HCC)的可行性。检索了截至2021年4月9日的PubMed、Embase、Medline和Cochrane图书馆。主要终点是≥3级并发症,次要终点是总生存期(OS)。对EBRT靶区、肝内与非肝内病变(如仅肝外转移或恶性血管受累)的研究进行了亚组分析。本荟萃分析纳入了11项涉及512例患者的研究。胃肠道、肝脏、血液学和皮肤学≥3级毒性的合并发生率分别为8.1%(95%置信区间(CI):4.8-13.5,I=0%)、12.9%(95%CI:7.1-22.1,I=22.4%)、9.1%(95%CI:3.8-20.3,I=51.3%)和6.8%(95%CI:3.8-11.7,I=0%)。靶向非肝内病变的研究中,合并的≥3级肝脏和血液学毒性发生率低于靶向肝内病变的研究(肝脏:3.3%对17.1%,P=0.041;血液学:3.3%对16.0%,P=0.078)。亚组间胃肠道和皮肤学≥3级并发症无显著差异。关于总生存期,联合治疗比非联合治疗更有益(优势比:3.3,95%CI:1.3-8.59,P=0.015)。一项研究报告了1例因肿瘤破裂和胃肠道出血导致的致命毒性病例。联合治疗可考虑应用于靶向转移性病变或局部血管受累情况。对于肝内病变,应考虑靶区大小和肝脏储备情况谨慎治疗。