Vaughn Samuel E, Strawn Jeffrey R, Poweleit Ethan A, Sarangdhar Mayur, Ramsey Laura B
Division of Child and Adolescent Psychiatry, Department of Pediatrics, Cincinnati Children's Hospital Medical Center, College of Medicine, University of Cincinnati, Cincinnati, OH 45229, USA.
Department of Psychiatry and Behavioral Neuroscience, College of Medicine, University of Cincinnati, Cincinnati, OH 45219, USA.
J Pers Med. 2021 Jun 29;11(7):615. doi: 10.3390/jpm11070615.
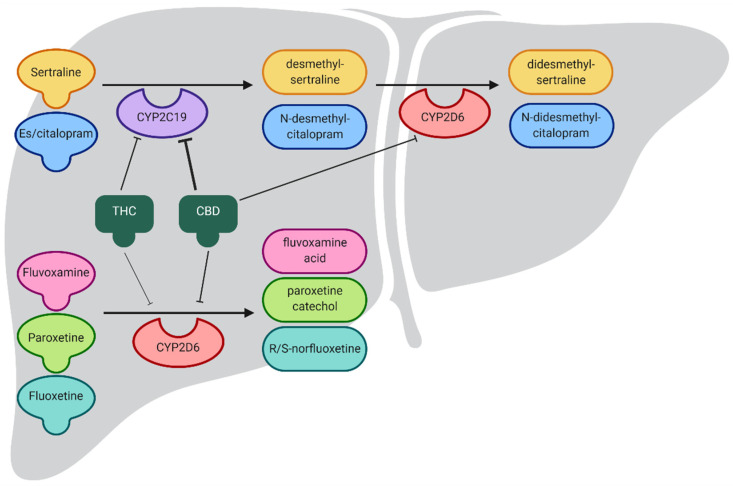
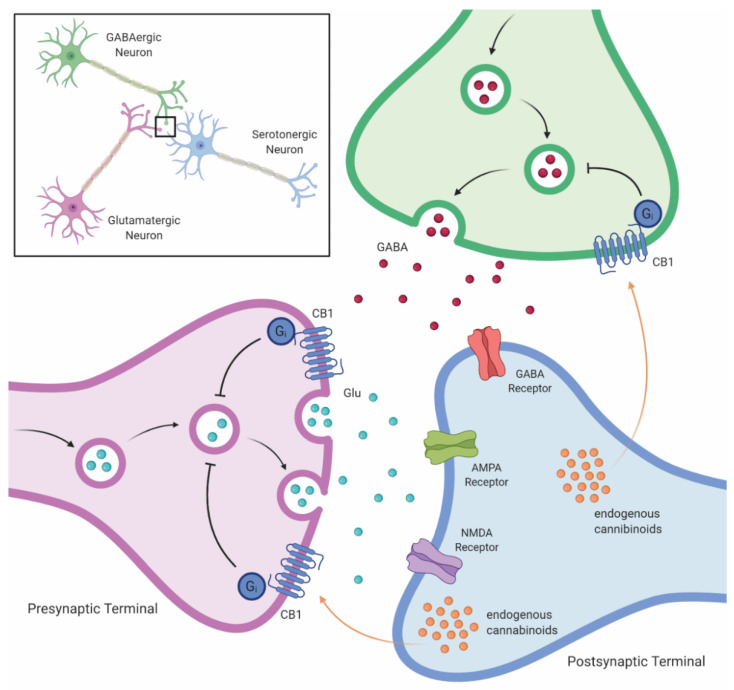
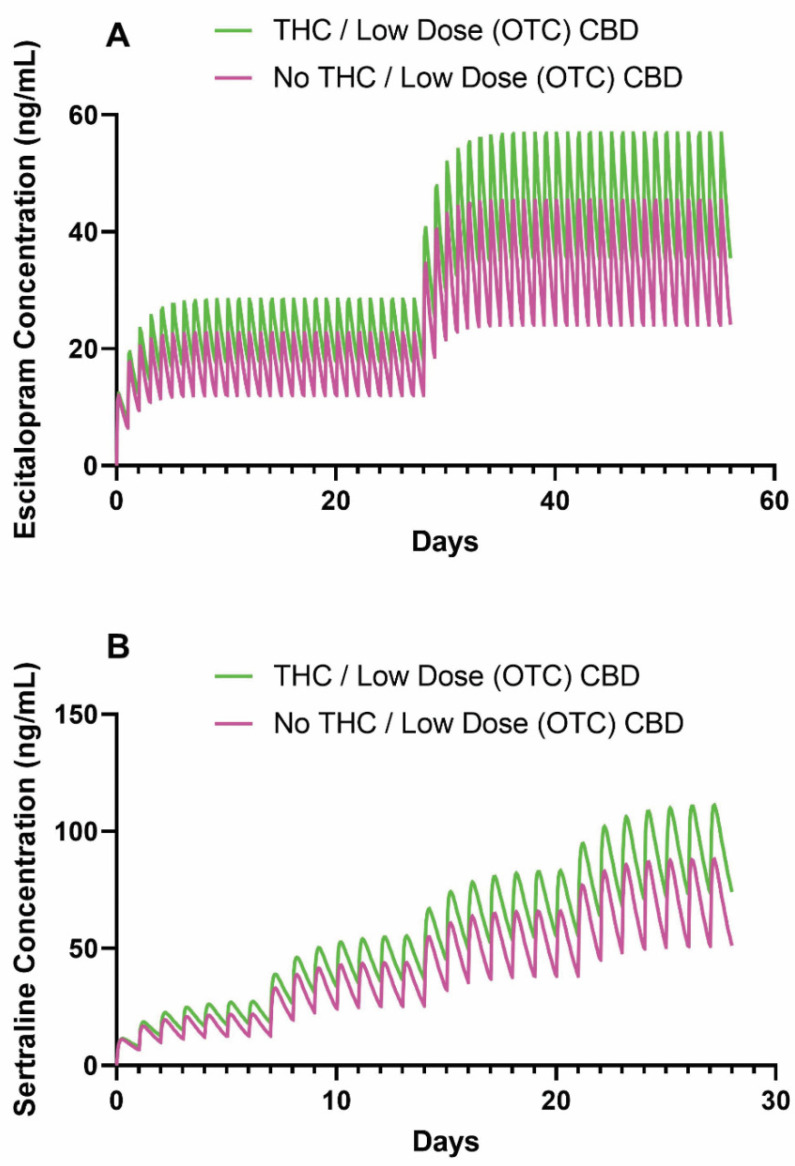
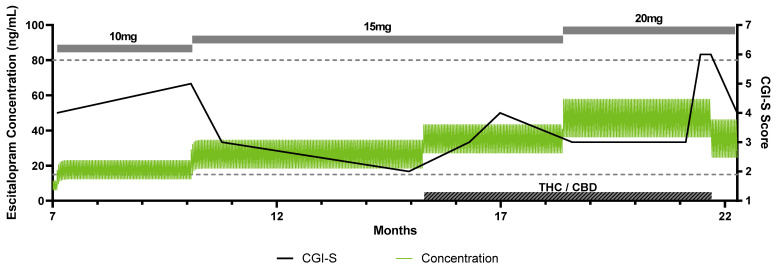
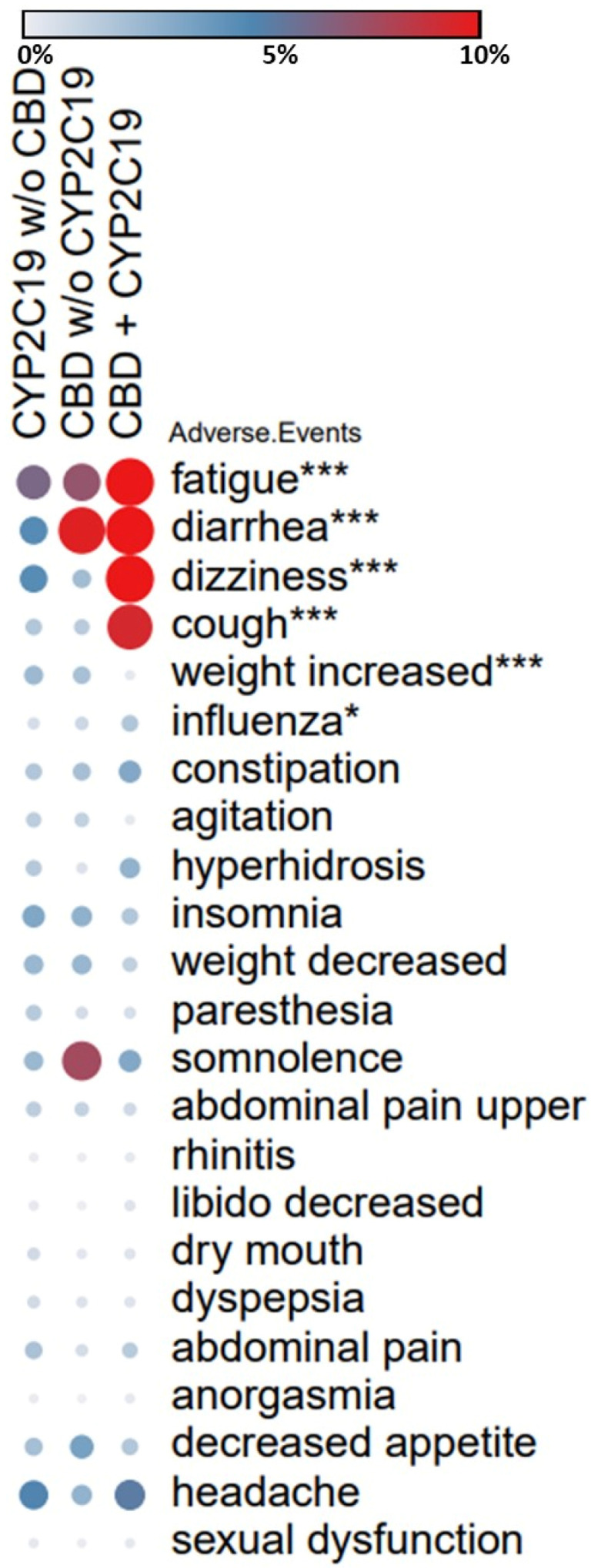
The neuropharmacology of marijuana, including its effects on selective serotonin reuptake inhibitor (SSRI)/antidepressant metabolism and the subsequent response and tolerability in youth, has received limited attention. We sought to (1) review clinically relevant pharmacokinetic (PK) and pharmacodynamic (PD) interactions between cannabinoids and selected SSRIs, (2) use PK models to examine the impact of cannabinoids on SSRI exposure (area under curve (AUC)) and maximum concentration (C) in adolescents, and (3) examine the frequency of adverse events reported when SSRIs and cannabinoids are used concomitantly. Cannabinoid metabolism, interactions with SSRIs, impact on relevant PK/PD pathways and known drug-drug interactions were reviewed. Then, the impact of tetrahydrocannabinol (THC) and cannabidiol (CBD) on exposure (AUC) and C for escitalopram and sertraline was modeled using pediatric PK data. Using data from the Food and Drug Administration Adverse Events Reporting System (FAERS), the relationship between CBD and CYP2C19-metabolized SSRIs and side effects was examined. Cannabis and CBD inhibit cytochrome activity, alter serotonergic transmission, and modulate SSRI response. In PK models, CBD and/or THC increases sertraline and es/citalopram concentrations in adolescents, and coadministration of CBD and CYP2C19-metabolized SSRIs increases the risk of cough, diarrhea, dizziness, and fatigue. Given the significant SSRI-cannabinoid interactions, clinicians should discuss THC and CBD use in youth prescribed SSRIs and be aware of the impact of initiating, stopping, or decreasing cannabinoid use as this may significantly affect es/citalopram and sertraline exposure.
大麻的神经药理学,包括其对选择性5-羟色胺再摄取抑制剂(SSRI)/抗抑郁药代谢的影响以及随后在青少年中的反应和耐受性,受到的关注有限。我们试图(1)回顾大麻素与选定的SSRI之间临床相关的药代动力学(PK)和药效学(PD)相互作用,(2)使用PK模型研究大麻素对青少年中SSRI暴露(曲线下面积(AUC))和最大浓度(C)的影响,以及(3)研究同时使用SSRI和大麻素时报告的不良事件频率。回顾了大麻素代谢、与SSRI的相互作用、对相关PK/PD途径的影响以及已知的药物-药物相互作用。然后,使用儿科PK数据模拟了四氢大麻酚(THC)和大麻二酚(CBD)对艾司西酞普兰和舍曲林的暴露(AUC)和C的影响。使用来自美国食品药品监督管理局不良事件报告系统(FAERS)的数据,研究了CBD与CYP2C19代谢的SSRI之间的关系以及副作用。大麻和CBD抑制细胞色素活性,改变5-羟色胺能传递,并调节SSRI反应。在PK模型中,CBD和/或THC会增加青少年中舍曲林和艾司/西酞普兰的浓度,同时使用CBD和CYP2C19代谢的SSRI会增加咳嗽、腹泻、头晕和疲劳的风险。鉴于SSRI与大麻素之间存在显著相互作用,临床医生应讨论在开具SSRI处方的青少年中使用THC和CBD的情况,并意识到开始、停止或减少大麻素使用的影响,因为这可能会显著影响艾司/西酞普兰和舍曲林的暴露。