Department of Laboratory Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China.
BMC Infect Dis. 2021 Jul 2;21(1):638. doi: 10.1186/s12879-021-06315-0.
Searching the risk factors for carbapenem-resistant Enterobacteriaceae (CRE) infection is important in clinical practice. In the present study, we aim to investigate bacterial characteristics of colonizing strains and their correlation with subsequent CRE infection.
Between May 2018 and January 2019, patients hospitalized in the department of haematology and intensive care unit (ICU) were screened for CRE by rectal swabs and monitored for the outcome of infection. We identified the species and carbapenemase-encoding genes of colonizing strains and performed antimicrobial susceptibility tests and multilocus sequence typing (MLST). Risk factors for subsequent CRE infections were ascertained by univariate and multivariable analysis.
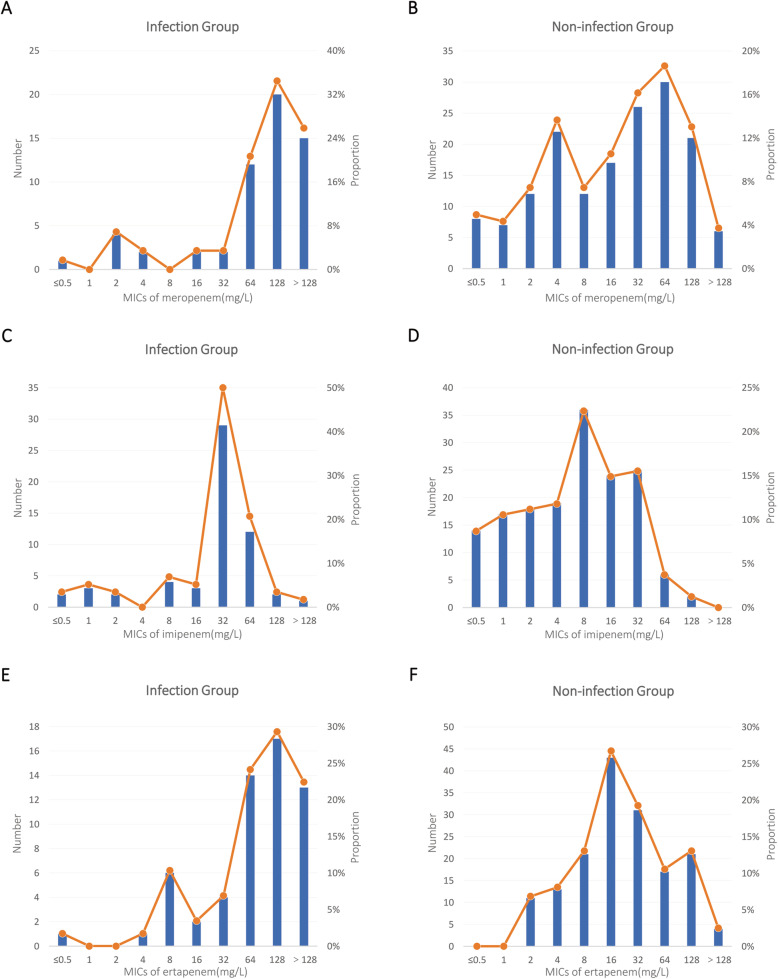
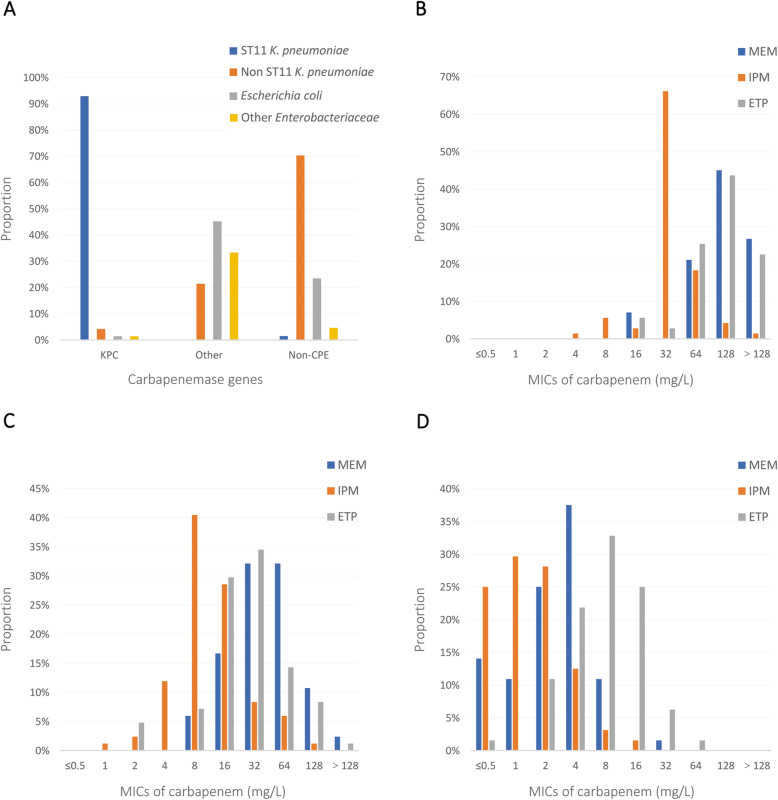
We collected a total of 219 colonizing strains from 153 patients. Klebsiella pneumoniae was the most abundant species, and MLST analysis showed rich diversity. K. pneumoniae carbapenemase (KPC) was predominant in the infection group (72.4%). In the non-infection group, 35.4% of strains were non-carbapenemase-producing CRE (NCP-CRE), and New Delhi metallo-β-lactamase (NDM) was predominant (42.2%). The rate of high-level carbapenem resistance (minimum inhibitory concentration [MIC] ≥ 64 mg/L for meropenem and ertapenem, ≥ 32 mg/L for imipenem) was remarkably higher in the infection group than in the non-infection group (P < 0.001). Univariate analysis showed that K. pneumoniae, high-level carbapenem resistance, CP-CRE and KPC-CRE were infection risk factors after CRE colonization. On multivariable analysis with different carbapenemase dichotomizations, KPC-CRE (adjusted odds ratio [aOR], 4.507; 95% confidence interval [CI], 1.339-15.171; P = 0.015) or imipenem MIC ≥ 32 mg/L (aOR, 9.515; 95% CI, 1.617-55.977; P = 0.013) were respectively identified as independent risk factors for subsequent infection.
Patients colonized with KPC-CRE or strains with an imipenem MIC ≥ 32 mg/L were at particularly high risk of subsequent CRE infections during their hospital stay.
在临床实践中,寻找碳青霉烯类耐药肠杆菌科(CRE)感染的危险因素非常重要。本研究旨在调查定植菌的细菌特征及其与随后 CRE 感染的相关性。
2018 年 5 月至 2019 年 1 月,对血液科和重症监护病房(ICU)住院患者进行直肠拭子筛查,以检测 CRE,并监测感染结局。我们鉴定定植菌的种属和碳青霉烯酶编码基因,并进行抗菌药物敏感性试验和多位点序列分型(MLST)。采用单因素和多因素分析确定随后发生 CRE 感染的危险因素。
我们从 153 名患者中共收集了 219 株定植菌。肺炎克雷伯菌是最丰富的种属,MLST 分析显示其多样性丰富。感染组中主要为产 KPC 酶肺炎克雷伯菌(72.4%)。非感染组中,35.4%的菌株为非产碳青霉烯酶 CRE(NCP-CRE),以新德里金属β-内酰胺酶(NDM)为主(42.2%)。感染组的高水平碳青霉烯类耐药率(美罗培南和厄他培南的最低抑菌浓度 [MIC]≥64mg/L,亚胺培南的 MIC≥32mg/L)显著高于非感染组(P<0.001)。单因素分析显示,肺炎克雷伯菌、高水平碳青霉烯类耐药、CP-CRE 和 KPC-CRE 是 CRE 定植后感染的危险因素。在不同碳青霉烯酶二分法的多因素分析中,KPC-CRE(调整优势比 [aOR],4.507;95%置信区间 [CI],1.339-15.171;P=0.015)或亚胺培南 MIC≥32mg/L(aOR,9.515;95%CI,1.617-55.977;P=0.013)分别被确定为随后感染的独立危险因素。
在住院期间,患者定植 KPC-CRE 或亚胺培南 MIC≥32mg/L 的菌株感染 CRE 的风险特别高。