Livermore David M
Norwich Medical School, University of East Anglia, Norwich, Norfolk NR4 7TJ, UK.
JAC Antimicrob Resist. 2021 Jun 15;3(Suppl 1):i5-i16. doi: 10.1093/jacamr/dlab052. eCollection 2021 Jun.
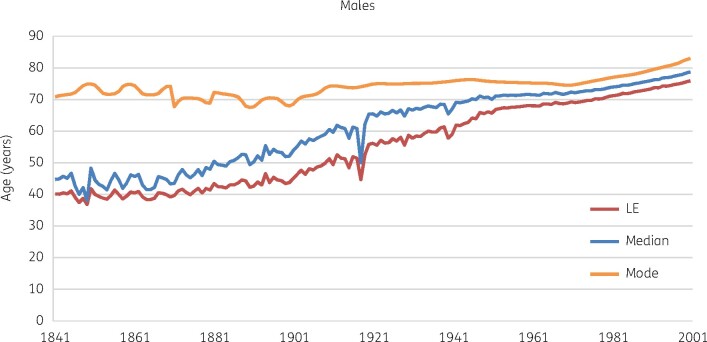
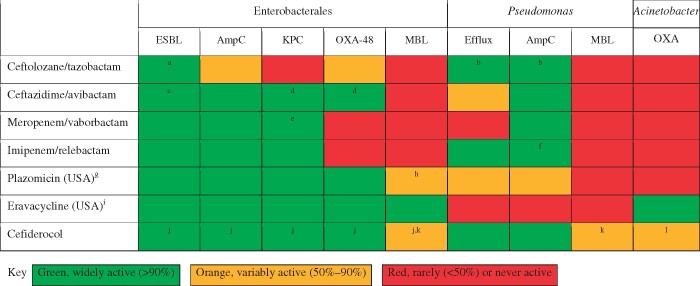
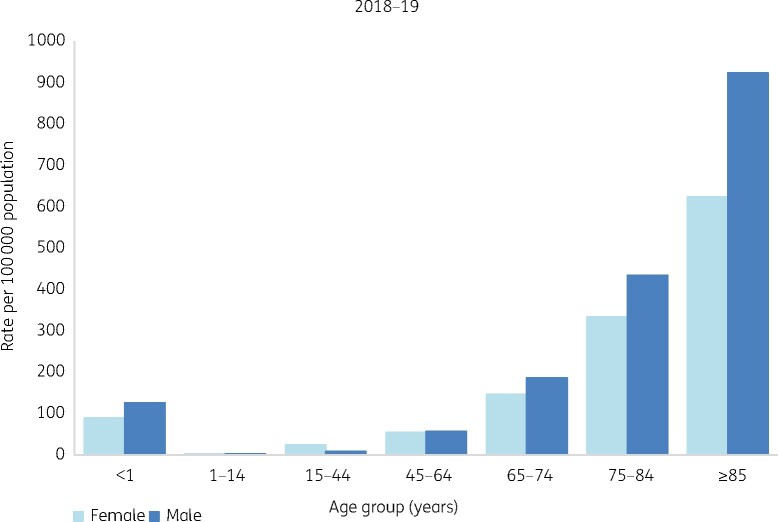
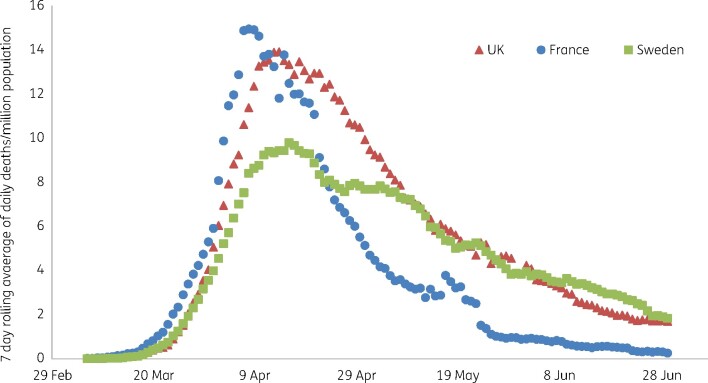
Antibiotics underpin the 'modern medicine' that has increased life expectancy, leading to societies with sizeable vulnerable elderly populations who have suffered disproportionately during the current COVID-19 pandemic. Governments have responded by shuttering economies, limiting social interactions and refocusing healthcare. There are implications for antibiotic resistance both during and after these events. During spring 2020, COVID-19-stressed ICUs relaxed stewardship, perhaps promoting resistance. Counterpoised to this, more citizens died at home and total hospital antibiotic use declined, reducing selection pressure. Restricted travel and social distancing reduced community import and transmission of resistant bacteria, though hard data are lacking. The future depends on the vaccines now being deployed. Unequivocal vaccine success should allow a swift return to normality. Vaccine failure followed by extended and successful non-pharmaceutical suppression may lead to the same point, but only after some delay, and with indefinite travel restrictions; sustainability is doubtful. Alternatively, failure of vaccines and control measures may prompt acceptance that we must live with the virus, as in the prolonged 1889-94 'influenza' (or coronavirus OC43) pandemic. Vaccine failure scenarios, particularly those accepting 'learning to live with the virus', favour increased outpatient management of non-COVID-19 infections using oral and long antibiotics. Ultimately, all models-except those envisaging societal collapse-suggest that COVID-19 will be controlled and that hospitals will revert to pre-2020 patterns with a large backlog of non-COVID-19 patients awaiting treatment. Clearing this will increase workloads, stresses, nosocomial infections, antibiotic use and resistance. New antibiotics, including cefiderocol, are part of the answer.
抗生素是“现代医学”的基石,它延长了人类的预期寿命,使得社会中出现了大量易受伤害的老年人群体,而这些人群在当前的新冠疫情中遭受了 disproportionately 的痛苦。各国政府采取的应对措施包括关闭经济、限制社交互动以及重新调整医疗保健重点。这些事件期间及之后对抗生素耐药性都会产生影响。在 2020 年春季,不堪重负的新冠重症监护病房放松了管理,这可能会促进耐药性的产生。与此相反,更多公民在家中死亡,医院抗生素的总体使用量下降,从而降低了选择压力。尽管缺乏确凿数据,但旅行限制和社交距离减少了耐药菌的社区输入和传播。未来取决于目前正在部署的疫苗。明确的疫苗成功应能使迅速恢复正常。疫苗失败,随后进行长期且成功的非药物抑制,可能也会导致同样的结果,但会有所延迟,且旅行限制将不确定;其可持续性令人怀疑。或者,疫苗和控制措施的失败可能会促使人们接受我们必须与病毒共存,就像在 1889 - 1894 年漫长的“流感”(或冠状病毒 OC43)大流行期间那样。疫苗失败的情况,尤其是那些接受“学会与病毒共存”的情况,有利于增加使用口服和长效抗生素对非新冠感染进行门诊管理。最终,除了那些设想社会崩溃的模型外,所有模型都表明新冠疫情将得到控制,医院将恢复到 2020 年之前的模式,有大量非新冠患者等待治疗。清理这些积压患者将增加工作量、压力、医院感染、抗生素使用和耐药性。包括头孢地尔在内的新型抗生素是解决方案的一部分。