Department of Medicine, University of Montréal, CRCHUM, Québec, Canada.
The George Institute for Global Health, University of New South Wales, Sydney, NSW, Australia.
Diabetologia. 2021 Sep;64(9):2012-2025. doi: 10.1007/s00125-021-05491-7. Epub 2021 Jul 6.
AIMS/HYPOTHESIS: Type 2 diabetes increases the risk of cardiovascular and renal complications, but early risk prediction could lead to timely intervention and better outcomes. Genetic information can be used to enable early detection of risk.
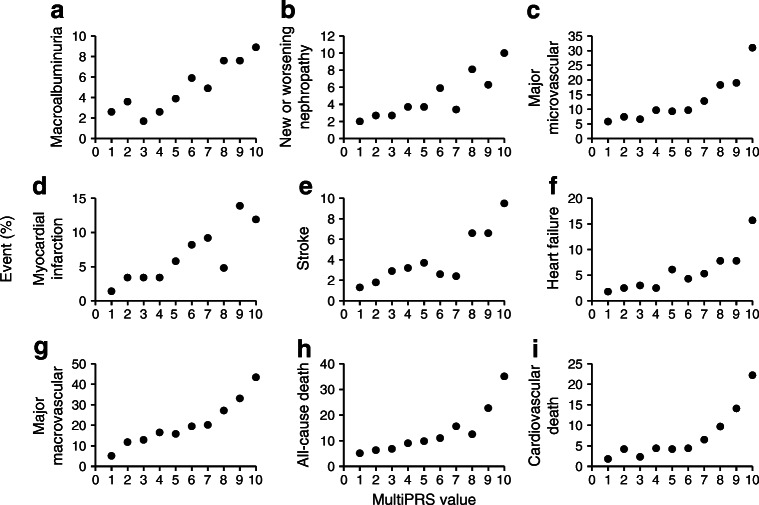
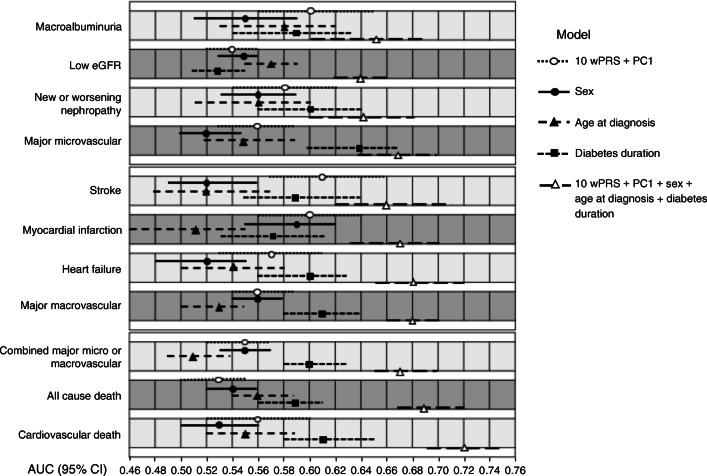
We developed a multi-polygenic risk score (multiPRS) that combines ten weighted PRSs (10 wPRS) composed of 598 SNPs associated with main risk factors and outcomes of type 2 diabetes, derived from summary statistics data of genome-wide association studies. The 10 wPRS, first principal component of ethnicity, sex, age at onset and diabetes duration were included into one logistic regression model to predict micro- and macrovascular outcomes in 4098 participants in the ADVANCE study and 17,604 individuals with type 2 diabetes in the UK Biobank study.
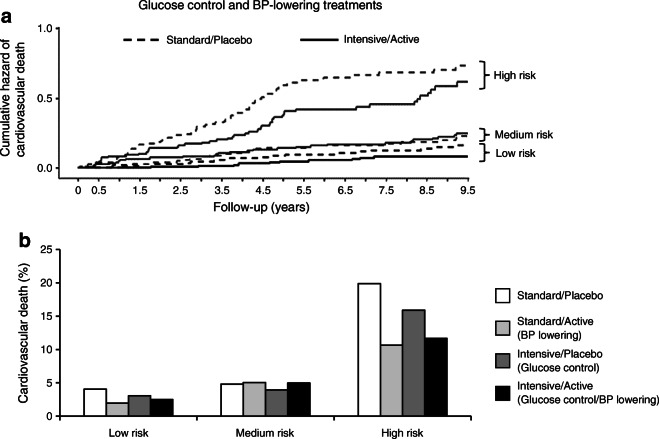
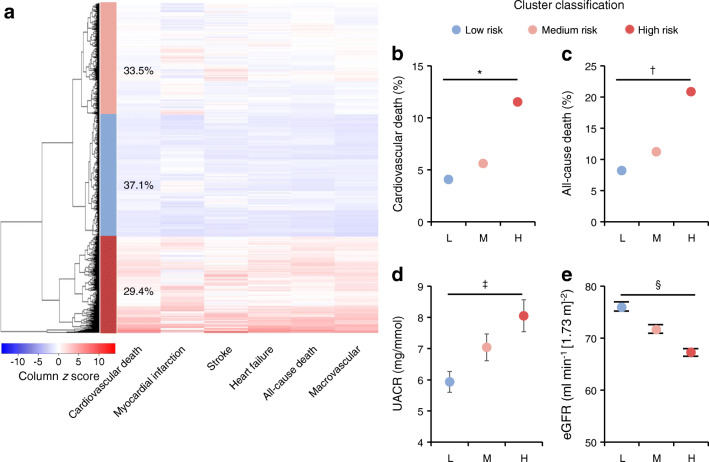
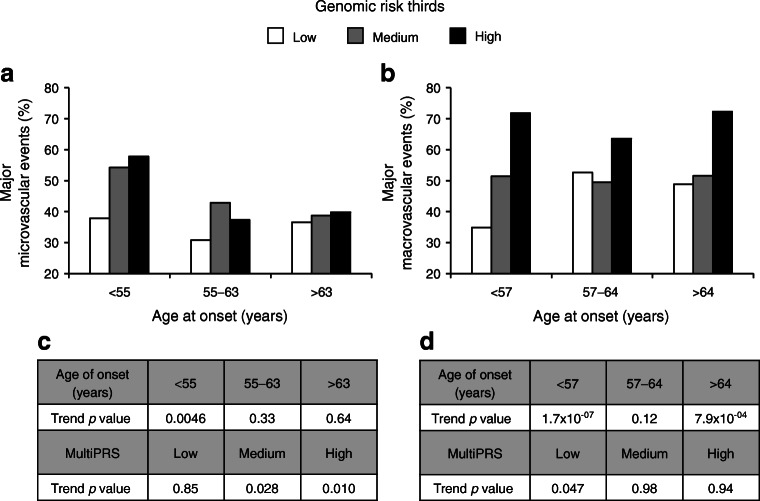
The model showed a similar predictive performance for cardiovascular and renal complications in different cohorts. It identified the top 30% of ADVANCE participants with a mean of 3.1-fold increased risk of major micro- and macrovascular events (p = 6.3 × 10 and p = 9.6 × 10, respectively) and a 4.4-fold (p = 6.8 × 10) higher risk of cardiovascular death. While in ADVANCE overall, combined intensive blood pressure and glucose control decreased cardiovascular death by 24%, the model identified a high-risk group in whom it decreased the mortality rate by 47%, and a low-risk group in whom it had no discernible effect. High-risk individuals had the greatest absolute risk reduction with a number needed to treat of 12 to prevent one cardiovascular death over 5 years.
CONCLUSIONS/INTERPRETATION: This novel multiPRS model stratified individuals with type 2 diabetes according to risk of complications and helped to target earlier those who would receive greater benefit from intensive therapy.
目的/假设:2 型糖尿病会增加心血管和肾脏并发症的风险,但早期风险预测可以实现及时干预和改善预后。遗传信息可用于早期发现风险。
我们开发了一个多基因风险评分(multiPRS),该评分由与 2 型糖尿病主要风险因素和结局相关的 598 个 SNP 组成的 10 个加权 PRS(10 wPRS)组成,这些 SNP 来自全基因组关联研究的汇总统计数据。将 10 wPRS、种族、性别、发病年龄和糖尿病病程的第一主成分纳入一个逻辑回归模型,以预测 ADVANCE 研究的 4098 名参与者和 UK Biobank 研究的 17604 名 2 型糖尿病患者的微血管和大血管结局。
该模型在不同队列中对心血管和肾脏并发症具有相似的预测性能。它确定了 ADVANCE 参与者中前 30%的个体具有更高的主要微血管和大血管事件风险(平均风险比为 3.1 倍,p=6.3×10-5 和 p=9.6×10-5,分别),心血管死亡风险增加 4.4 倍(p=6.8×10-5)。尽管在 ADVANCE 研究中,强化血压和血糖控制综合降低了 24%的心血管死亡风险,但该模型确定了一个高危组,其中死亡率降低了 47%,而一个低危组则没有明显效果。高危个体的绝对风险降低最大,每 12 例患者接受治疗可预防 5 年内发生 1 例心血管死亡。
结论/解释:这种新型多PRS 模型根据并发症风险对 2 型糖尿病患者进行分层,并有助于针对那些从强化治疗中获益最大的患者进行早期治疗。