Goldberger Jeffrey J, Subačius Haris, Marroquin Oscar C, Beau Scott L, Simonson Jay
University of Miami Miller School of Medicine Miami FL.
Division of Research and Optimal Patient Care American College of Surgeons Chicago IL.
J Am Heart Assoc. 2021 Jul 20;10(14):e019017. doi: 10.1161/JAHA.120.019017. Epub 2021 Jul 6.
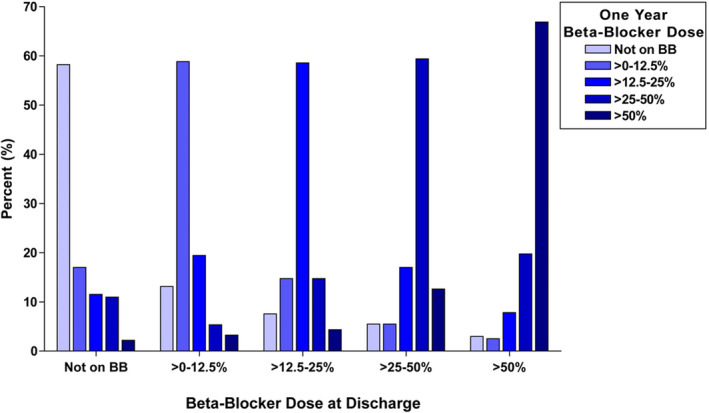
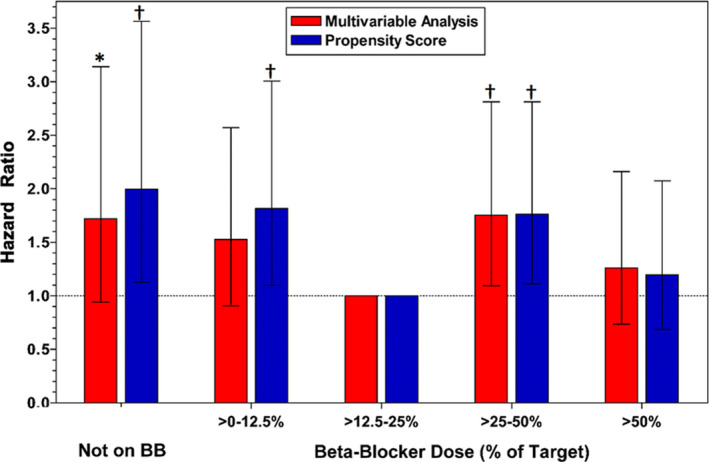
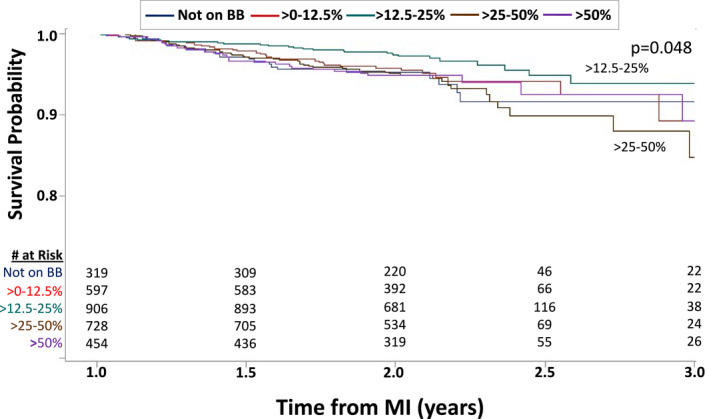
Background Although beta-blockers are recommended following myocardial infarction (MI), the benefits of long-term treatment have not been established. The study's aim was to evaluate beta-blocker efficacy by dose in 1-year post-MI survivors. Methods and Results The OBTAIN (Outcomes of Beta-Blocker Therapy After Myocardial Infarction) registry included 7057 patients with acute MI, with 6077 one-year survivors. For this landmark analysis, beta-blocker dose status was available in 3004 patients and analyzed by use (binary) and dose at 1 year after MI. Doses were classified as no beta-blocker and >0% to 12.5%, >12.5% to 25%, >25% to 50%, and >50% of target doses used in randomized clinical trials. Age was 63 to 64 years, and approximately two thirds were men. Median follow-up duration was 1.05 years (interquartile range, 0.98-1.22). When analyzed dichotomously, beta-blocker therapy was not associated with improved survival. When analyzed by dose, propensity score analysis showed significantly increased mortality in the no-beta-blocker group (hazard ratio,1.997; 95% CI, 1.118-3.568; <0.02), the >0% to 12.5% group (hazard ratio, 1.817; 95% CI, 1.094-3.016; <0.02), and the >25% to 50% group (hazard ratio, 1.764; 95% CI, 1.105-2.815; <0.02), compared with the >12.5% to 25% dose group. The mortality in the full-dose group was not significantly higher (hazard ratio, 1.196; 95% CI, 0.687-2.083). In subgroup analyses, only history of congestive heart failure demonstrated significant interaction with beta-blocker effects on survival. Conclusions This analysis suggests that patients treated with >12.5% to 25% of the target dose used in prior randomized clinical trials beyond 1 year after MI may have enhanced survival compared with no beta-blocker and other beta-blocker doses. A new paradigm for post-MI beta-blocker therapy is needed that addresses which patients should be treated, for how long, and at what dose.
尽管心肌梗死(MI)后推荐使用β受体阻滞剂,但长期治疗的益处尚未明确。本研究旨在评估心肌梗死后1年存活患者中β受体阻滞剂按剂量的疗效。
OBTAIN(心肌梗死后β受体阻滞剂治疗的结果)注册研究纳入了7057例急性心肌梗死患者,其中6077例为1年存活者。对于这项标志性分析,3004例患者有β受体阻滞剂剂量状态信息,并在心肌梗死后1年按使用情况(二分法)和剂量进行分析。剂量分为未使用β受体阻滞剂、使用剂量为随机临床试验中目标剂量的>0%至12.5%、>12.5%至25%、>25%至50%以及>50%。患者年龄为63至64岁,约三分之二为男性。中位随访时间为1.05年(四分位间距,0.98 - 1.22年)。二分法分析时,β受体阻滞剂治疗与生存率改善无关。按剂量分析时,倾向评分分析显示,与使用剂量为目标剂量的>12.5%至25%组相比,未使用β受体阻滞剂组(风险比,1.997;95%可信区间,1.118 - 3.568;P<0.02)、>0%至12.5%组(风险比,1.817;95%可信区间,1.094 - 3.016;P<0.02)以及>25%至50%组(风险比,1.764;95%可信区间,1.105 - 2.815;P<0.02)的死亡率显著升高。全剂量组的死亡率没有显著升高(风险比,1.196;95%可信区间,0.687 - 2.083)。在亚组分析中,只有充血性心力衰竭病史显示与β受体阻滞剂对生存的影响存在显著交互作用。
本分析表明,与未使用β受体阻滞剂及其他β受体阻滞剂剂量相比,心肌梗死后1年以上使用剂量为既往随机临床试验中目标剂量的>12.5%至25%进行治疗的患者可能有更高的生存率。需要一种新的心肌梗死后β受体阻滞剂治疗模式,以解决哪些患者应接受治疗、治疗多长时间以及使用何种剂量的问题。