Office of Cooperative Reproductive Health, Department of Family and Preventive Medicine, University of Utah School of Medicine, 375 Chipeta Way, Suite A, Salt Lake City, UT, 84108, USA.
International Institute for Restorative Reproductive Medicine, London, UK.
BMC Pregnancy Childbirth. 2021 Jul 7;21(1):495. doi: 10.1186/s12884-021-03946-8.
Restorative reproductive medicine (RRM) seeks to identify and correct underlying causes and factors contributing to infertility and reproductive dysfunction. Many components of RRM are highly suitable for primary care practice. We studied the outcomes amongst couples who received restorative reproductive medicine treatment for infertility in a primary care setting.
Two family physicians in Massachusetts trained in a systematic approach to RRM (natural procreative technology, or NaProTechnology) treated couples with infertility. We retrospectively reviewed the characteristics, diagnoses, treatments, and outcomes for all couples treated during the years 1989 to 2014. We compared pregnancy and live birth by clinical characteristics using Kaplan-Meier analysis. We employed the Fleming-Harrington weighted Renyi test or the logrank test to compare the cumulative proportion with pregnancy or with live birth.
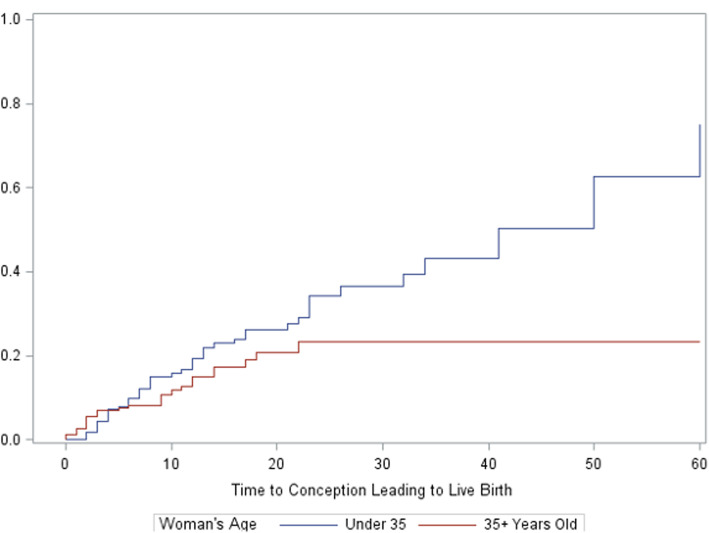
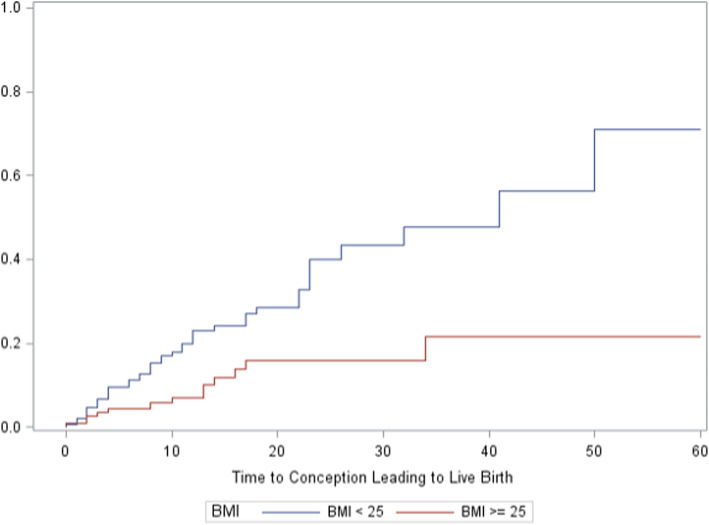
Among 370 couples beginning treatment for infertility, the mean age was 34.8 years, the mean prior time trying to conceive was 2.7 years, and 27% had a prior live birth. The mean number of diagnoses per couple was 4.9. Treatment components included fertility tracking with the Creighton Model FertilityCare System (80%); medications to enhance cervical mucus production (81%), to stimulate ovulation (62%), or to support the luteal phase (75%); and referral to female laparoscopy by a surgeon specializing in endometriosis (46%). The cumulative live birth rate at 2 years was 29% overall; this was significantly higher for women under age 35 (34%), and for women with body mass index < 25 (40%). There were 2 sets of twins and no higher-order multiple gestations. Of the 63 births with data available, 58 (92%) occurred at term.
Family physicians can provide a RRM approach for infertility to identify underlying causes and promote healthy term live births. Younger women and women with body mass index < 25 are more likely to have a live birth.
修复性生殖医学(RRM)旨在识别和纠正导致不孕和生殖功能障碍的潜在原因和因素。RRM 的许多组成部分非常适合初级保健实践。我们研究了在初级保健环境中接受修复性生殖医学治疗不孕的夫妇的结果。
马萨诸塞州的两位家庭医生接受了系统的 RRM 治疗(自然生殖技术,或 NaProTechnology),治疗不孕夫妇。我们回顾性地审查了 1989 年至 2014 年期间所有接受治疗的夫妇的特征、诊断、治疗和结果。我们使用 Kaplan-Meier 分析比较了临床特征的妊娠和活产率。我们采用 Fleming-Harrington 加权 Renyi 检验或对数秩检验比较妊娠或活产的累积比例。
在 370 对开始治疗不孕的夫妇中,平均年龄为 34.8 岁,平均尝试受孕时间为 2.7 年,27%有过活产。每对夫妇的平均诊断数为 4.9。治疗包括使用 Creighton 模型生育保健系统进行生育跟踪(80%);使用药物促进宫颈粘液分泌(81%)、刺激排卵(62%)或支持黄体期(75%);以及由专门治疗子宫内膜异位症的外科医生转介进行女性腹腔镜检查(46%)。2 年时的总活产率为 29%;35 岁以下的女性(34%)和 BMI<25 的女性(40%)的活产率显著更高。有 2 对双胞胎,没有更高阶的多胎妊娠。在可获得数据的 63 例分娩中,58 例(92%)足月分娩。
家庭医生可以为不孕提供 RRM 方法,以确定潜在原因并促进健康足月活产。年轻女性和 BMI<25 的女性更有可能活产。