School of Medicine, China Medical University, Taichung, 404, Taiwan.
Department of Orthopedic Surgery, China Medical University Hospital, Taichung, 404, Taiwan.
J Orthop Surg Res. 2021 Jul 7;16(1):441. doi: 10.1186/s13018-021-02575-3.
Metacarpal shaft fractures are a common hand trauma. The current surgical fixation options for such fractures include percutaneous Kirschner wire pinning and nonlocking and locking plate fixation. Although bone plate fixation, compared with Kirschner wire pinning, has superior fixation ability, a consensus has not been reached on whether the bone plate is better placed on the dorsal or lateral side.
The purpose of this study was to evaluate the fixation of locking and regular bone plates on the dorsal and lateral sides of a metacarpal shaft fracture.
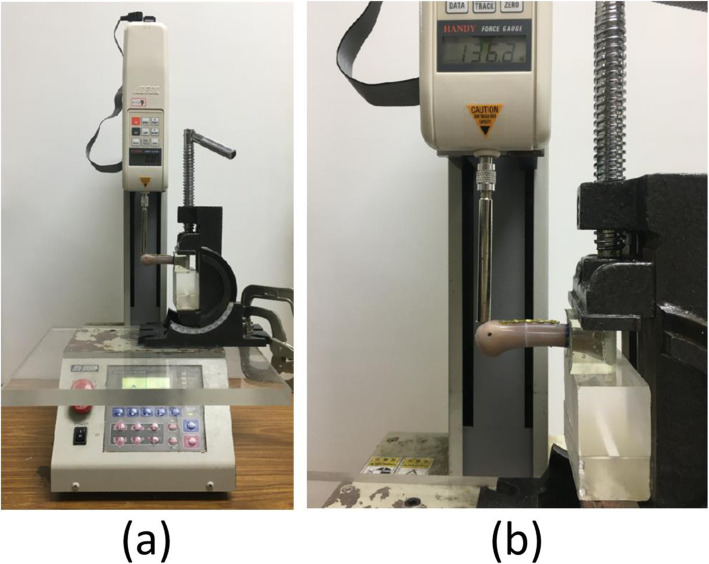
Thirty-five artificial metacarpal bones were used in the experiment. Metacarpal shaft fractures were created using a saw blade, which were then treated with four types of fixation as follows: (1) a locking plate with four locking bicortical screws on the dorsal side (LP_D); (2) a locking plate with four locking bicortical screws on the lateral side (LP_L); (3) a regular plate with four regular bicortical screws on the dorsal side (RP_D); (4) a regular plate with four regular bicortical screws on the lateral side (RP_D); and (5) two K-wires (KWs). All specimens were tested through cantilever bending tests on a material testing system. The maximum fracture force and stiffness of the five fixation types were determined based on the force-displacement data. The maximum fracture force and stiffness of the specimens with metacarpal shaft fractures were first analyzed using one-way analysis of variance and Tukey's test.
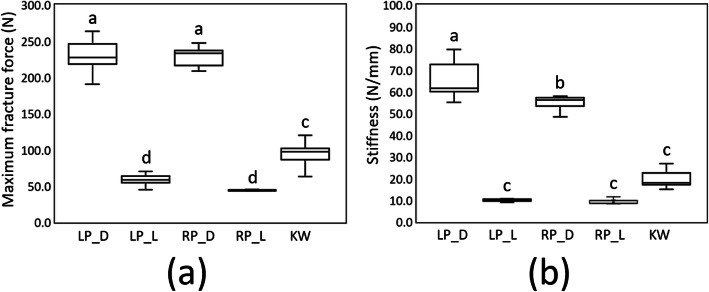
The maximum fracture force results of the five types of metacarpal shaft fracture were as follows: LP_D group (230.1 ± 22.8 N, mean ± SD) ≅ RP_D group (228.2 ± 13.4 N) > KW group (94.0 ± 17.4 N) > LP_L group (59.0 ± 7.9 N) ≅ RP_L group (44.5 ± 3.4 N). In addition, the stiffness results of the five types of metacarpal shaft fracture were as follows: LP_D group (68.7 ± 14.0 N/mm) > RP_D group (54.9 ± 3.2 N/mm) > KW group (20.7 ± 5.8 N/mm) ≅ LP_L group (10.6 ± 1.7 N/mm) ≅ RP_L group (9.4 ± 1.2 N/mm).
According to our results, the mechanical strength offered by lateral plate fixation of a metacarpal shaft fracture is so low that even KW fixation can offer relatively superior mechanical strength; this is regardless of whether a locking or nonlocking plate is used for lateral plate fixation. Such fixation can reduce the probability of extensor tendon adhesion. Nevertheless, our results indicated that when lateral plate fixation is used for fixating a metacarpal shaft fracture in a clinical setting, whether the mechanical strength offered by such fixation would be strong enough to support bone union remains questionable.
掌骨干骨折是手部常见的创伤。目前此类骨折的手术固定选择包括经皮克氏针固定和非锁定及锁定钢板固定。虽然钢板固定与克氏针固定相比具有更好的固定能力,但对于钢板应放置在掌骨背侧还是掌侧,尚未达成共识。
本研究旨在评估掌骨干骨折掌骨背侧和掌侧锁定钢板和普通钢板的固定效果。
实验共使用 35 根人工掌骨。使用锯片制作掌骨干骨折模型,然后采用以下 4 种固定方式进行治疗:(1)掌骨背侧 4 枚锁定双皮质螺钉的锁定钢板(LP_D);(2)掌骨背侧 4 枚锁定双皮质螺钉的锁定钢板(LP_L);(3)掌骨背侧 4 枚普通双皮质螺钉的普通钢板(RP_D);(4)掌骨掌侧 4 枚普通双皮质螺钉的普通钢板(RP_L);(5)2 枚克氏针(KWs)。所有标本均在材料测试系统上进行悬臂弯曲试验。根据力-位移数据确定 5 种固定类型的最大骨折力和刚度。首先使用单因素方差分析和 Tukey 检验分析掌骨干骨折 5 种固定类型的最大骨折力。
5 种掌骨干骨折的最大骨折力结果如下:LP_D 组(230.1 ± 22.8 N,均值 ± 标准差)≈RP_D 组(228.2 ± 13.4 N)>KW 组(94.0 ± 17.4 N)>LP_L 组(59.0 ± 7.9 N)≈RP_L 组(44.5 ± 3.4 N)。此外,5 种掌骨干骨折的刚度结果如下:LP_D 组(68.7 ± 14.0 N/mm)>RP_D 组(54.9 ± 3.2 N/mm)>KW 组(20.7 ± 5.8 N/mm)≈LP_L 组(10.6 ± 1.7 N/mm)≈RP_L 组(9.4 ± 1.2 N/mm)。
根据我们的结果,掌骨干骨折掌侧钢板固定的力学强度如此之低,即使使用克氏针固定也能提供相对较好的力学强度;无论使用锁定钢板还是非锁定钢板进行掌侧钢板固定均是如此。这种固定方式可以降低伸肌腱粘连的概率。然而,我们的研究结果表明,在临床应用掌骨干骨折掌侧钢板固定时,这种固定方式提供的力学强度是否足以支持骨折愈合仍存在疑问。