Department of Pediatrics, Critical Care Section, Seattle Children's Hospital, Seattle, WA, USA.
Department of Pediatrics, Baylor College of Medicine, Houston, TX, USA.
Pediatr Nephrol. 2022 Jan;37(1):189-197. doi: 10.1007/s00467-021-05177-7. Epub 2021 Jul 7.
Ongoing measures to improve pediatric continuous kidney replacement therapy (CKRT) have lowered mortality rates, shifting the focus to survivor functional status. While septic acute kidney injury generates new morbidity in pediatric critically ill patients, acquired morbidities and functional status of CKRT population are unknown. We predicted that CKRT survivors are at risk for new morbidity and would have worse functional status at PICU discharge compared to baseline, and aimed to describe associated factors.
Retrospective cohort study over 24 months of CKRT patients surviving to PICU discharge in a quaternary children's hospital. Functional outcome was determined by Functional Status Scale (FSS).
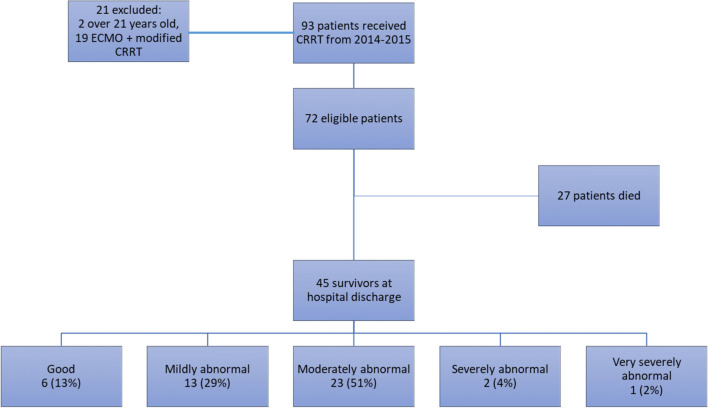
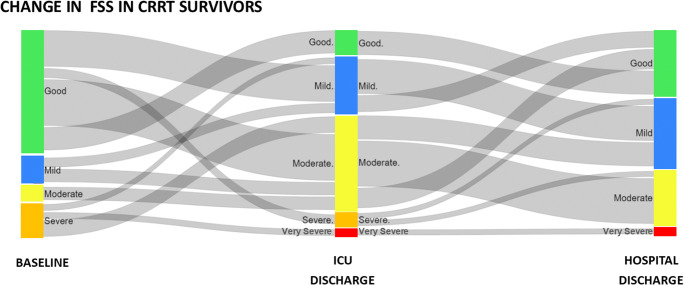
FSS scores were higher at PICU and hospital discharge compared to baseline. Of 45 CKRT survivors, 31 (69%) had worse FSS score at PICU discharge and 51% had new morbidity (≥3 increase in FSS); majority qualified as moderate to severe disability (FSS ≥10). Four patients (9%) had new tracheostomy, 3 (7%) were ventilator dependent, and 10 (22%) were dialysis dependent. Most (23/45, 51%) required outpatient rehabilitation. Cumulative days on sedation, controlled for illness severity, were independently associated with worse FSS at PICU discharge (aOR 25.18 (3.73, 169.92)). In adjusted analyses, duration of sedation was associated with new morbidity, while neurologic comorbidity, percent fluid overload at CKRT start, and nonrenal comorbidity were associated with moderate to severe disability at PICU discharge when controlled for baseline FSS.
CKRT survivors, with new morbidity and worse functional outcomes at PICU discharge, are a newly described vulnerable population requiring targeted follow-up. Deliberate decrease of sedation exposure in patients with decreased clearance due to organ dysfunction needs to be studied as a modifiable risk factor.
为提高儿科连续性肾脏替代治疗(CKRT)的水平,目前已采取多项措施,这使得病死率降低,转而关注幸存者的功能状态。虽然脓毒症引起的急性肾损伤会增加儿科危重症患者的新发病,但 CKRT 人群的获得性疾病和功能状态尚不清楚。我们预测 CKRT 幸存者存在发生新发病的风险,与基线相比,他们在 PICU 出院时的功能状态更差,并旨在描述相关因素。
对一家四级儿童医院 24 个月内存活至 PICU 出院的 CKRT 患者进行回顾性队列研究。通过功能状态量表(FSS)确定功能结局。
与基线相比,PICU 和出院时的 FSS 评分更高。在 45 例 CKRT 幸存者中,31 例(69%)在 PICU 出院时的 FSS 评分更差,51%有新发病(FSS 增加≥3);大多数(23/45,51%)患者为中重度残疾(FSS≥10)。4 例(9%)患者新行气管切开术,3 例(7%)患者依赖呼吸机,10 例(22%)患者依赖透析。大多数(23/45,51%)患者需要门诊康复。校正疾病严重程度后,镇静持续时间与 PICU 出院时 FSS 更差相关(调整后 OR 25.18(3.73,169.92))。在调整分析中,镇静时间与新发病相关,而神经合并症、CKRT 开始时的液体超负荷百分比以及非肾脏合并症与 PICU 出院时的中重度残疾相关,同时控制了基线 FSS。
CKRT 幸存者在 PICU 出院时存在新发病和更差的功能结局,是一个新描述的脆弱人群,需要有针对性的随访。由于器官功能障碍导致清除率降低的患者,应减少镇静暴露,这需要作为一个可改变的危险因素进行研究。