Ernst Jochen, Friedrich Michael, Vehling Sigrun, Koch Uwe, Mehnert-Theuerkauf Anja
Department of Medical Psychology and Medical Sociology, University Hospital Leipzig, Leipzig, Germany.
Department of Medical Psychology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Front Psychol. 2021 Jun 23;12:660588. doi: 10.3389/fpsyg.2021.660588. eCollection 2021.
The Distress Thermometer (DT) is a validated and widely used screening tool to identify clinically relevant distress in cancer patients. It is unclear, to which extend subjectively perceived distress measured by the DT is related to objective burden (mental disorder). We therefore examine the co-occurrence of a mental disorder for different DT thresholds and explore the diagnostic properties of the DT in detecting a mental disorder.
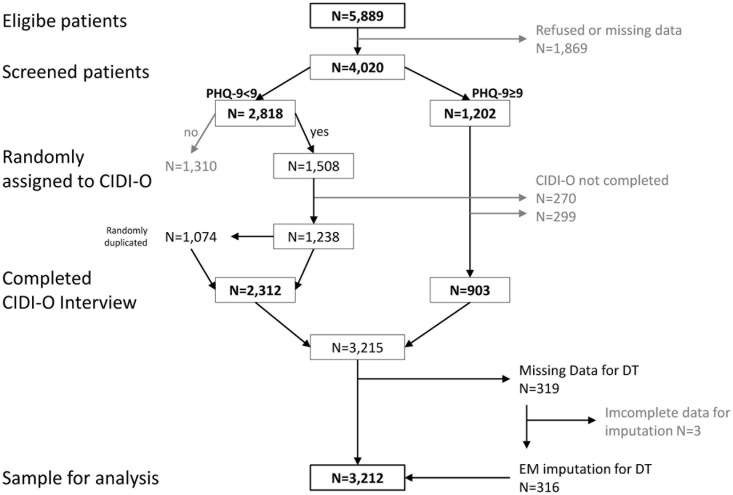
In this multicenter cross-sectional study, we included 4,020 patients with mixed cancer diagnoses. After selection of relevant cases, weighting procedure and imputation of missing data we evaluated the data of = 3,212 patients. We used the DT to assess perceived distress and the standardized Composite International Diagnostic Interview for Oncology (CIDI-O) to assess the 4-week prevalence of mental disorders. The association between distress and any mental disorder (MD) is calculated using Pearson correlations. Relative risks for MD in patients with/without distress and the co-occurrence of distress and MD were calculated with Poisson regression. To assess the operating characteristics between distress and MD, we present the area under the curve (AUC).
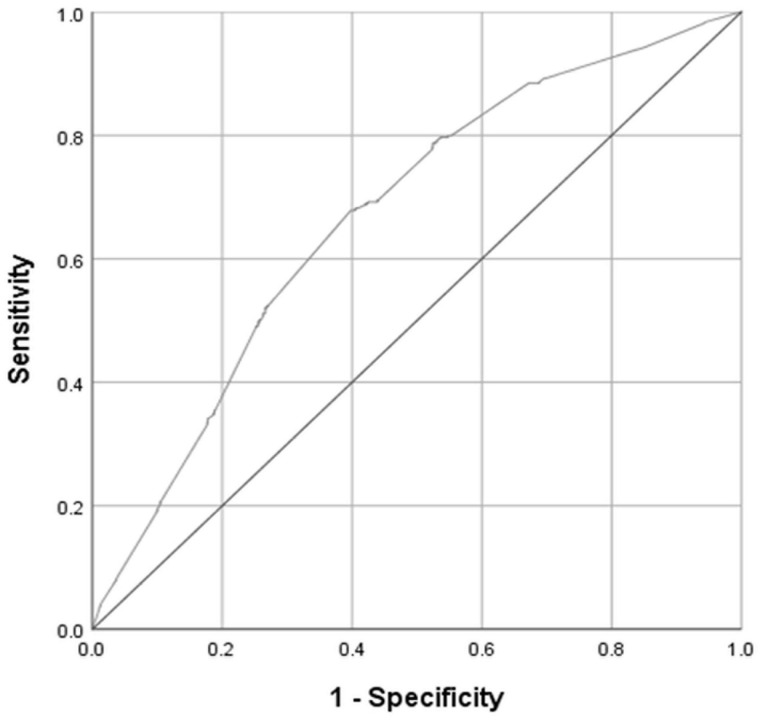
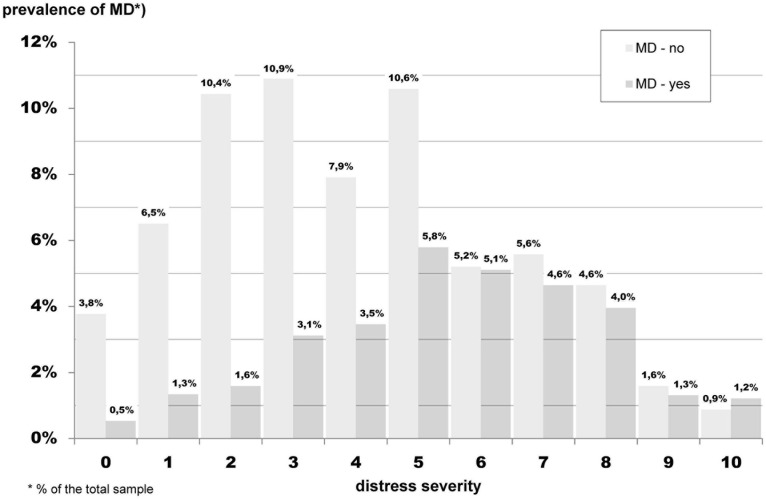
22.9% of the participants had a cut-off DT level of ≥5 and were affected by MD. Each level of distress co-occurs with MD. The proportion of patients diagnosed with MD was not greater than the proportion of patients without MD until distress levels of DT = 6 were reached. The correlation between DT and MD was = 0.27. The ROC-analysis shows the area under curve (AUC) = 0.67, which is classified as unsatisfactory. With increasing distress severity, patients are not more likely to have a mental disorder.
Our results suggests viewing and treating cancer-related distress as a relatively distinct psychological entity. Cancer-related distress may be associated with an increased risk for a mental disorder and vice versa, but the overlap of both concepts is very moderate.
苦恼温度计(DT)是一种经过验证且广泛使用的筛查工具,用于识别癌症患者临床上相关的苦恼。目前尚不清楚,通过DT测量的主观感知苦恼在多大程度上与客观负担(精神障碍)相关。因此,我们研究了不同DT阈值下精神障碍的共现情况,并探讨了DT在检测精神障碍方面的诊断特性。
在这项多中心横断面研究中,我们纳入了4020例患有混合癌症诊断的患者。在选择相关病例、进行加权程序和缺失数据插补后,我们评估了3212例患者的数据。我们使用DT评估感知到的苦恼,并使用标准化的国际肿瘤诊断访谈问卷(CIDI-O)评估精神障碍的4周患病率。使用Pearson相关性计算苦恼与任何精神障碍(MD)之间的关联。使用Poisson回归计算有/无苦恼的患者患MD的相对风险以及苦恼与MD的共现情况。为了评估苦恼与MD之间的操作特征,我们展示了曲线下面积(AUC)。
22.9%的参与者DT临界值≥5且患有MD。每个苦恼水平都与MD共现。在DT = 6的苦恼水平之前,被诊断患有MD的患者比例不高于未患MD的患者比例。DT与MD之间的相关性为 = 0.27。ROC分析显示曲线下面积(AUC) = 0.67,被归类为不理想。随着苦恼严重程度的增加,患者患精神障碍的可能性并不更高。
我们的结果表明,应将癌症相关苦恼视为一个相对独特的心理实体。癌症相关苦恼可能与精神障碍风险增加相关,反之亦然,但这两个概念的重叠程度非常适中。