GVM Care & Research Maria Cecilia Hospital, Cotignola, Italy.
Cardiovascular Department, ASST Santi Paolo e Carlo, Milan, Italy.
Geroscience. 2021 Oct;43(5):2215-2229. doi: 10.1007/s11357-021-00409-y. Epub 2021 Jul 14.
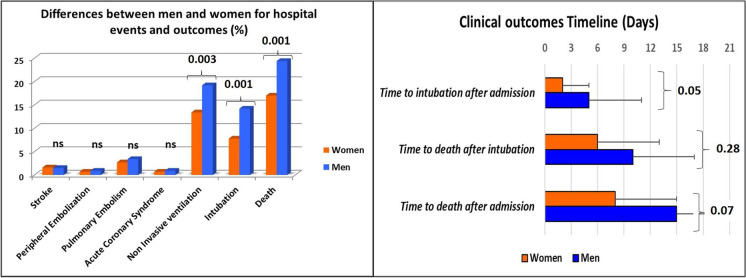
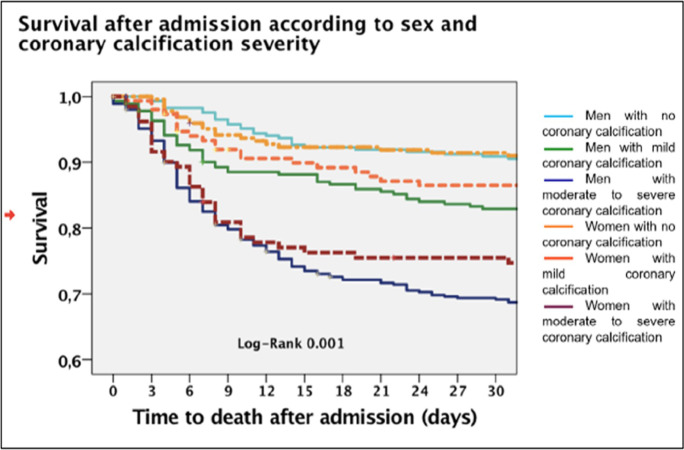
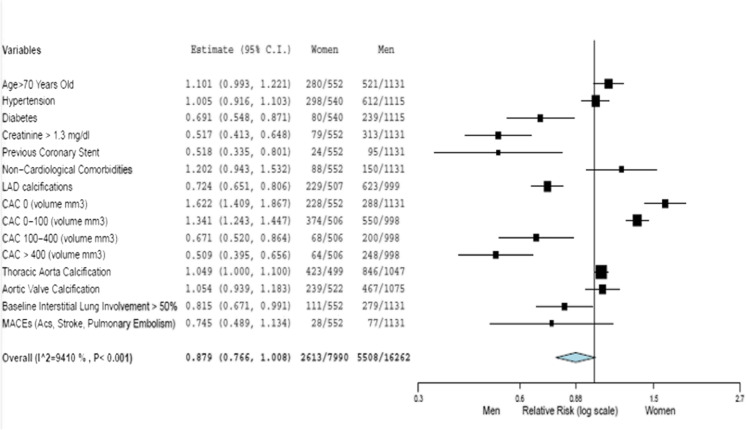
Recent clinical and demographical studies on COVID-19 patients have demonstrated that men experience worse outcomes than women. However, in most cases, the data were not stratified according to gender, limiting the understanding of the real impact of gender on outcomes. This study aimed to evaluate the disaggregated in-hospital outcomes and explore the possible interactions between gender and cardiovascular calcifications. Data was derived from the sCORE-COVID-19 registry, an Italian multicentre registry that enrolled COVID-19 patients who had undergone a chest computer tomography scan on admission. A total of 1683 hospitalized patients (mean age 67±14 years) were included. Men had a higher prevalence of cardiovascular comorbidities, a higher pneumonia extension, more coronary calcifications (63% vs.50.9%, p<0.001), and a higher coronary calcium score (391±847 vs. 171±479 mm, p<0.001). Men experienced a significantly higher mortality rate (24.4% vs. 17%, p=0.001), but the death event tended to occur earlier in women (15±7 vs. 8±7 days, p= 0.07). Non-survivors had a higher coronary, thoracic aorta, and aortic valve calcium score. Female sex, a known independent predictor of a favorable outcome in SARS-CoV2 infection, was not protective in women with a coronary calcification volume greater than 100 mm. There were significant differences in cardiovascular comorbidities and vascular calcifications between men and women with SARS-CoV2 pneumonia. The differences in outcomes can be at least partially explained by the different cardiovascular profiles. However, women with poor outcomes had the same coronary calcific burden as men. The presumed favorable female sex bias in COVID-19 must therefore be reviewed in the context of comorbidities, especially cardiovascular ones.
最近针对 COVID-19 患者的临床和人口学研究表明,男性的预后比女性差。然而,在大多数情况下,数据并未按性别分层,这限制了对性别对结局实际影响的理解。本研究旨在评估住院期间的细分结局,并探讨性别与心血管钙化之间可能存在的相互作用。数据来自 sCORE-COVID-19 登记处,这是一个意大利多中心登记处,纳入了入院时接受胸部计算机断层扫描的 COVID-19 患者。共纳入 1683 例住院患者(平均年龄 67±14 岁)。男性具有更高的心血管合并症患病率、更高的肺炎扩展程度、更多的冠状动脉钙化(63% vs.50.9%,p<0.001)和更高的冠状动脉钙评分(391±847 vs. 171±479 mm,p<0.001)。男性的死亡率显著更高(24.4% vs. 17%,p=0.001),但女性的死亡事件发生得更早(15±7 天 vs. 8±7 天,p=0.07)。非幸存者的冠状动脉、胸主动脉和主动脉瓣钙评分更高。女性是 SARS-CoV2 感染有利结局的已知独立预测因素,但在冠状动脉钙化体积大于 100mm 的女性中没有保护作用。SARS-CoV2 肺炎患者中,男性和女性在心血管合并症和血管钙化方面存在显著差异。结局的差异至少可以部分解释为不同的心血管特征。然而,预后不良的女性具有与男性相同的冠状动脉钙化负担。因此,在考虑合并症,特别是心血管合并症时,必须重新审视 COVID-19 中假定的女性有利性别偏见。