Department of Renal Medicine, Clinical Research Center for Rare Diseases, "Aldo e Cele Daccò": Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Ranica, Bergamo, Italy.
Unit of Nephrology and Dialysis, Azienda Socio-Sanitaria Territoriale Papa Giovanni XXIII, Bergamo, Italy.
PLoS Med. 2021 Jul 14;18(7):e1003691. doi: 10.1371/journal.pmed.1003691. eCollection 2021 Jul.
Angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) prevent microalbuminuria in normoalbuminuric type 2 diabetic patients. We assessed whether combined therapy with the 2 medications may prevent microalbuminuria better than ACE inhibitor or ARB monotherapy.
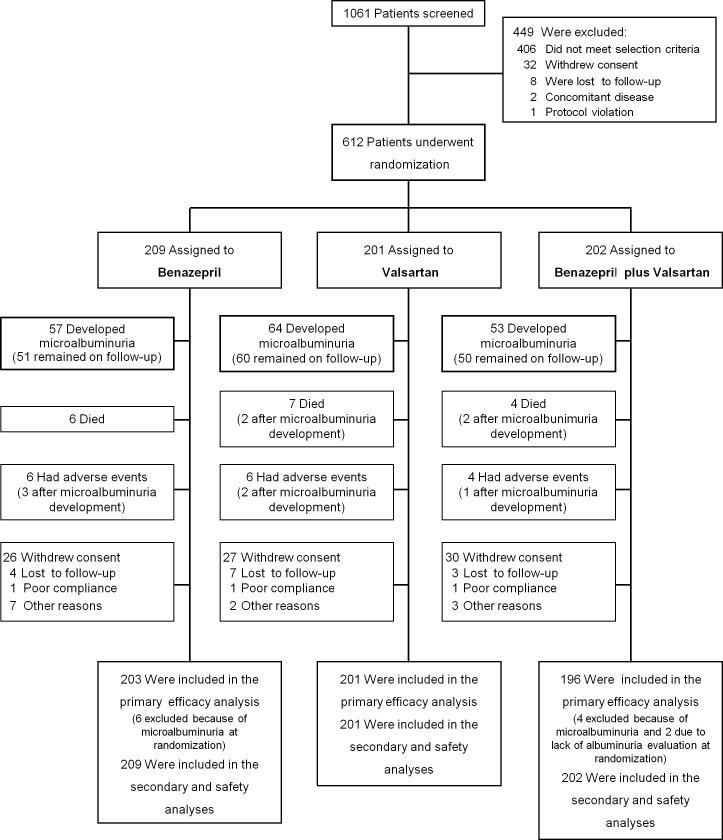
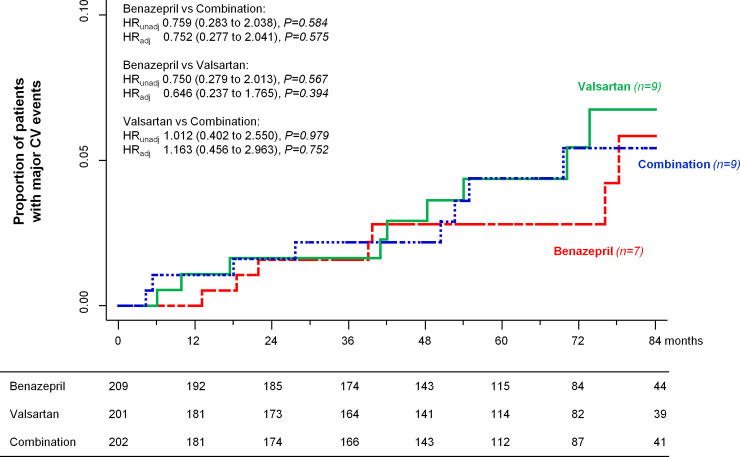
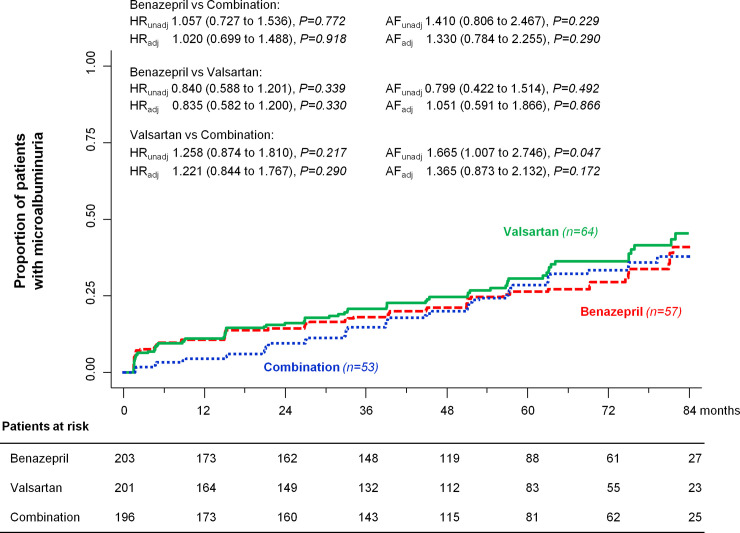
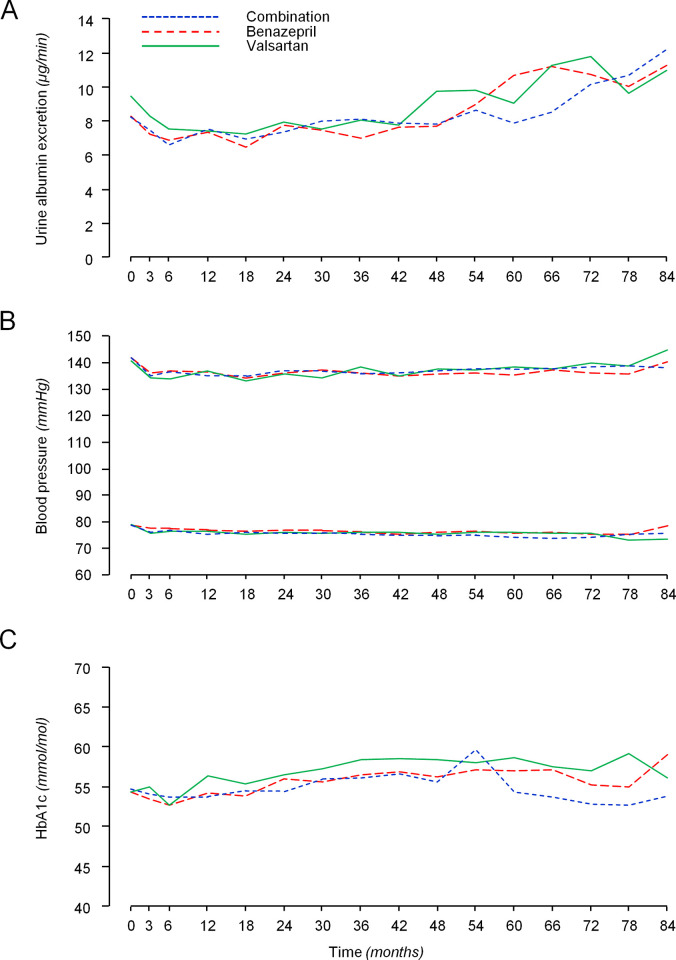
VARIETY was a prospective, randomized, open-label, blinded endpoint (PROBE) trial evaluating whether, at similar blood pressure (BP) control, combined therapy with benazepril (10 mg/day) and valsartan (160 mg/day) would prevent microalbuminuria more effectively than benazepril (20 mg/day) or valsartan (320 mg/day) monotherapy in 612 type 2 diabetic patients with high-normal albuminuria included between July 2007 and April 2013 by the Istituto di Ricerche Farmacologiche Mario Negri IRCCS and 8 diabetology or nephrology units in Italy. Time to progression to microalbuminuria was the primary outcome. Analyses were intention to treat. Baseline characteristics were similar among groups. During a median [interquartile range, IQR] follow-up of 66 [42 to 83] months, 53 patients (27.0%) on combination therapy, 57 (28.1%) on benazepril, and 64 (31.8%) on valsartan reached microalbuminuria. Using an accelerated failure time model, the estimated acceleration factors were 1.410 (95% CI: 0.806 to 2.467, P = 0.229) for benazepril compared to combination therapy, 0.799 (95% CI: 0.422 to 1.514, P = 0.492) for benazepril compared to valsartan, and 1.665 (95% CI: 1.007 to 2.746, P = 0.047) for valsartan compared to combination therapy. Between-group differences in estimated acceleration factors were nonsignificant after adjustment for predefined confounders. BP control was similar across groups. All treatments were safe and tolerated well, with a slight excess of hyperkalemia and hypotension in the combination therapy group. The main study limitation was the lower than expected albuminuria at inclusion.
Risk/benefit profile of study treatments was similar. Dual renin-angiotensin system (RAS) blockade is not recommended as compared to benazepril or valsartan monotherapy for prevention of microalbuminuria in normoalbuminuric type 2 diabetic patients.
EudraCT 2006-005954-62; ClinicalTrials.gov NCT00503152.
血管紧张素转换酶(ACE)抑制剂和血管紧张素受体阻滞剂(ARB)可预防正常白蛋白尿 2 型糖尿病患者的微量白蛋白尿。我们评估了联合使用这两种药物是否比 ACE 抑制剂或 ARB 单药治疗更能预防微量白蛋白尿。
VARIETY 是一项前瞻性、随机、开放标签、盲终点(PROBE)试验,评估了在相似的血压(BP)控制下,联合使用贝那普利(10mg/天)和缬沙坦(160mg/天)是否比贝那普利(20mg/天)或缬沙坦(320mg/天)单药治疗更能有效预防 612 例高正常白蛋白尿的 2 型糖尿病患者的微量白蛋白尿,这些患者于 2007 年 7 月至 2013 年 4 月间由意大利 Mario Negri IRCCS 药物研究所和 8 个糖尿病或肾病学单位入选。进展为微量白蛋白尿的时间是主要终点。分析采用意向治疗。各组间的基线特征相似。在中位[四分位距,IQR]随访 66[42 至 83]个月期间,53 例(27.0%)联合治疗组、57 例(28.1%)贝那普利组和 64 例(31.8%)缬沙坦组达到微量白蛋白尿。使用加速失效时间模型,贝那普利与联合治疗相比的估计加速因子为 1.410(95%CI:0.806 至 2.467,P=0.229),贝那普利与缬沙坦相比的估计加速因子为 0.799(95%CI:0.422 至 1.514,P=0.492),缬沙坦与联合治疗相比的估计加速因子为 1.665(95%CI:1.007 至 2.746,P=0.047)。调整了预先设定的混杂因素后,组间估计的加速因子差异无统计学意义。各组间的血压控制相似。所有治疗均安全且耐受性良好,联合治疗组血钾升高和低血压的发生率略高。主要研究局限性在于纳入时的白蛋白尿低于预期。
研究治疗的风险/获益情况相似。与贝那普利或缬沙坦单药治疗相比,双重肾素-血管紧张素系统(RAS)阻断不推荐用于预防正常白蛋白尿 2 型糖尿病患者的微量白蛋白尿。
EudraCT 2006-005954-62;ClinicalTrials.gov NCT00503152。