Department of Environmental Health and Safety, Stanford University, Stanford CA.
Department of Radiology, University Medical Center Utrecht, Utrecht.
Invest Radiol. 2022 Jan 1;57(1):13-22. doi: 10.1097/RLI.0000000000000808.
Although the Agatston score is a commonly used quantification method, rescan reproducibility is suboptimal, and different CT scanners result in different scores. In 2007, McCollough et al (Radiology 2007;243:527-538) proposed a standard for coronary artery calcium quantification. Advancements in CT technology over the last decade, however, allow for improved acquisition and reconstruction methods. This study aims to investigate the feasibility of a reproducible reduced dose alternative of the standardized approach for coronary artery calcium quantification on state-of-the-art CT systems from 4 major vendors.
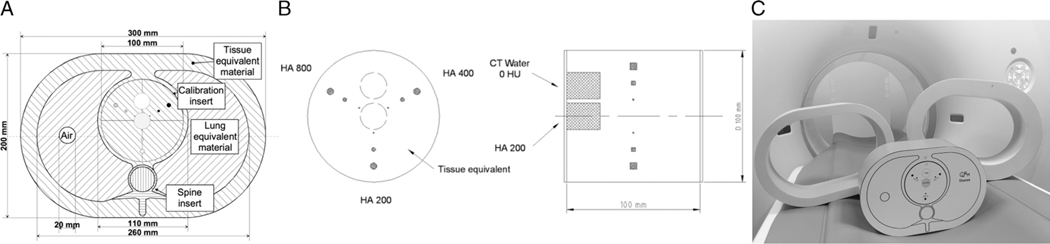
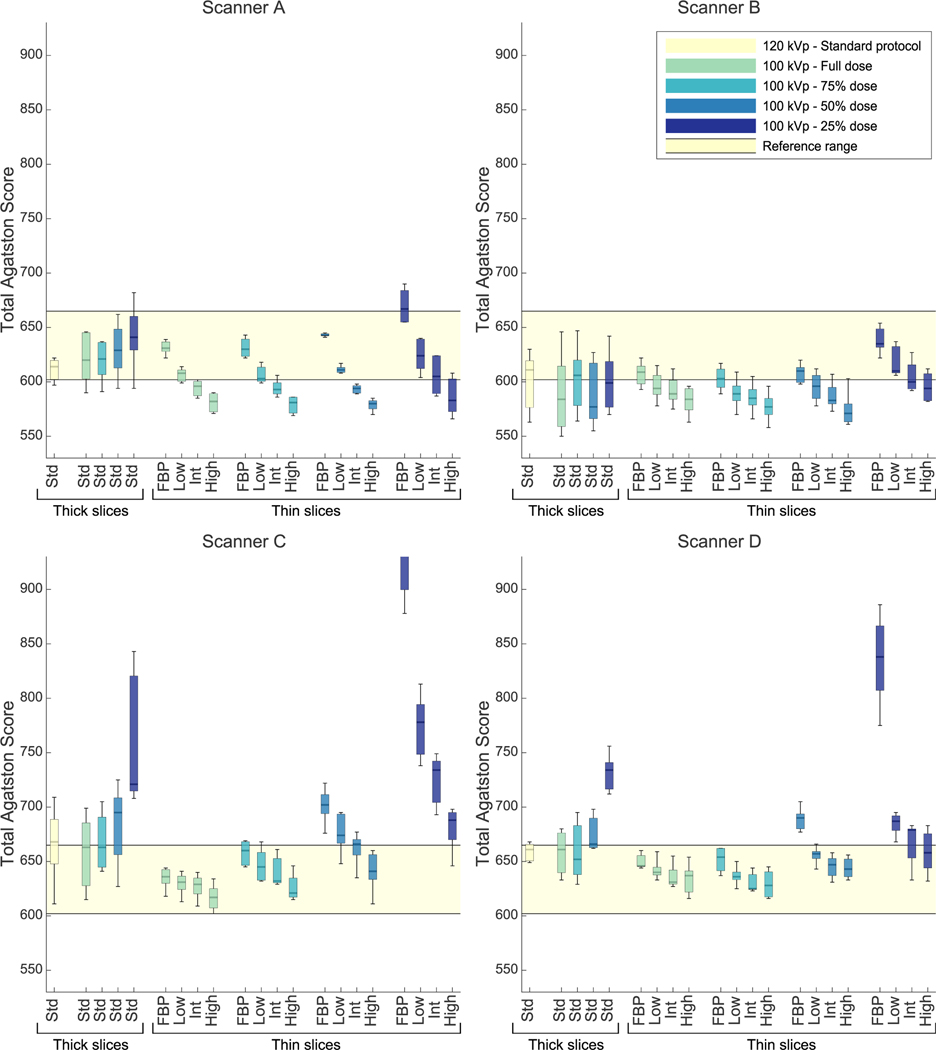
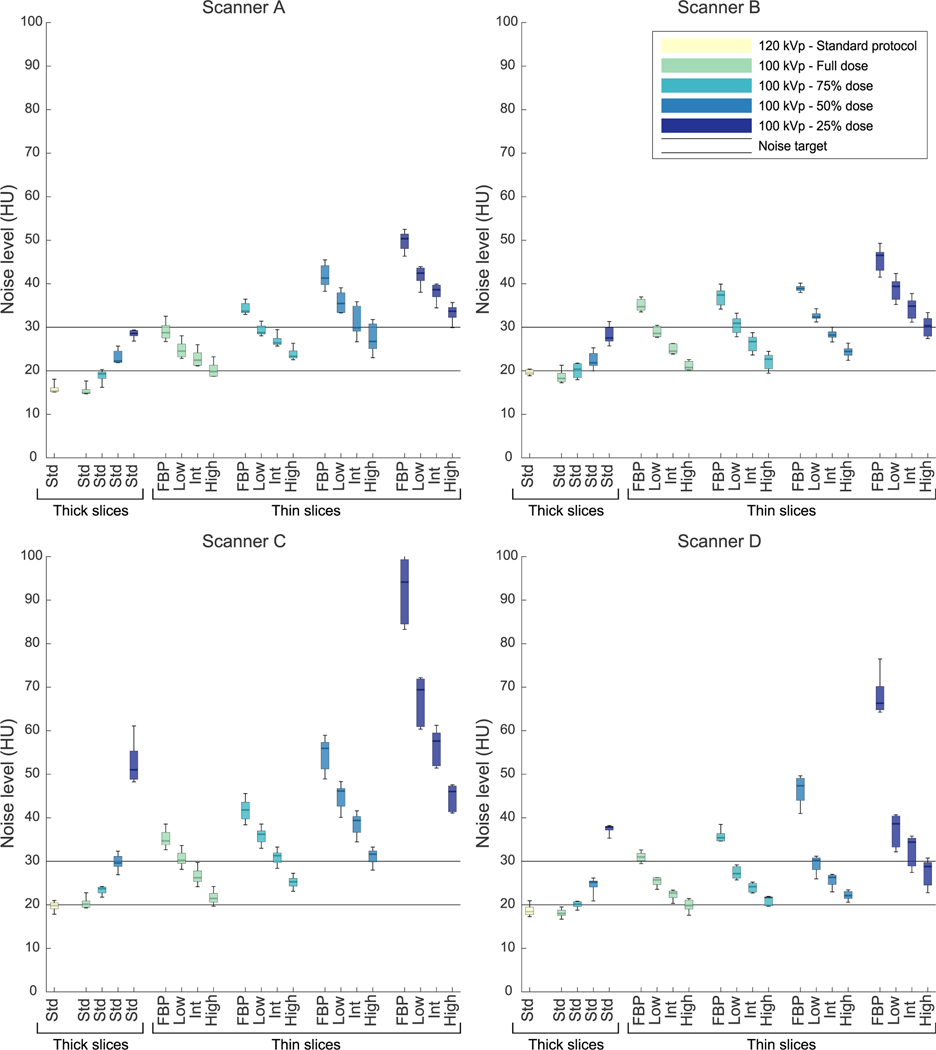
An anthropomorphic phantom containing 9 calcifications and 2 extension rings were used. Images were acquired with 4 state-of-the-art CT systems using routine protocols and a variety of tube voltages (80-120 kV), tube currents (100% to 25% dose levels), slice thicknesses (3/2.5 and 1/1.25 mm), and reconstruction techniques (filtered back projection and iterative reconstruction). Every protocol was scanned 5 times after repositioning the phantom to assess reproducibility. Calcifications were quantified as Agatston scores.
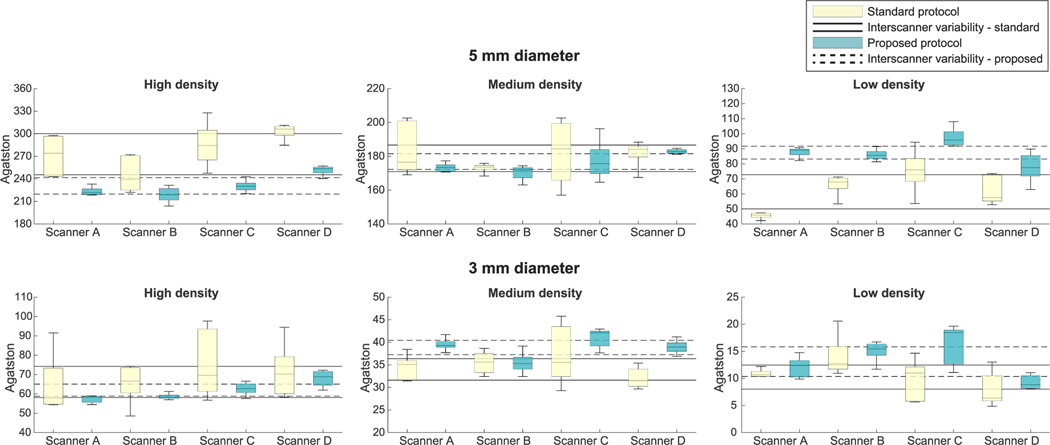
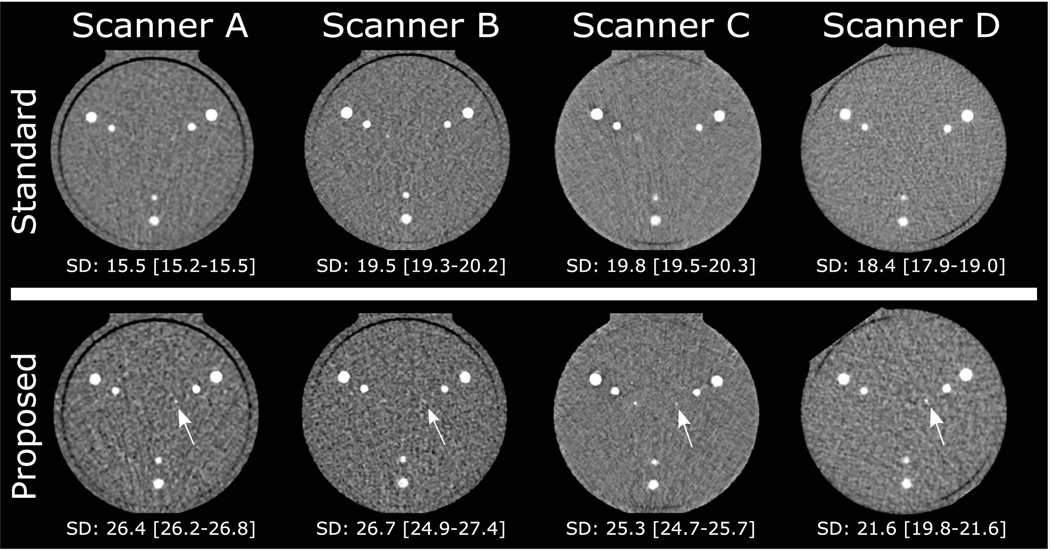
Reducing tube voltage to 100 kV, dose to 75%, and slice thickness to 1 or 1.25 mm combined with higher iterative reconstruction levels resulted in an on average 36% lower intrascanner variability (interquartile range) compared with the standard 120 kV protocol. Interscanner variability per phantom size decreased by 34% on average. With the standard protocol, on average, 6.2 ± 0.4 calcifications were detected, whereas 7.0 ± 0.4 were detected with the proposed protocol. Pairwise comparisons of Agatston scores between scanners within the same phantom size demonstrated 3 significantly different comparisons at the standard protocol (P < 0.05), whereas no significantly different comparisons arose at the proposed protocol (P > 0.05).
On state-of-the-art CT systems of 4 different vendors, a 25% reduced dose, thin-slice calcium scoring protocol led to improved intrascanner and interscanner reproducibility and increased detectability of small and low-density calcifications in this phantom. The protocol should be extensively validated before clinical use, but it could potentially improve clinical interscanner/interinstitutional reproducibility and enable more consistent risk assessment and treatment strategies.
尽管 Agatston 评分是一种常用的量化方法,但重新扫描的可重复性并不理想,并且不同的 CT 扫描仪会导致不同的评分。2007 年,McCollough 等人(Radiology 2007;243:527-538)提出了一种冠状动脉钙化定量的标准。然而,过去十年 CT 技术的进步允许采用改进的采集和重建方法。本研究旨在探讨在来自 4 家主要供应商的最先进 CT 系统上,使用一种可重复的、剂量降低的标准化方法替代冠状动脉钙化定量的可行性。
使用一个包含 9 个钙化和 2 个扩展环的人体模型。使用 4 台最先进的 CT 系统使用常规方案和各种管电压(80-120kV)、管电流(100%至 25%剂量水平)、层厚(3/2.5 和 1/1.25mm)和重建技术(滤波反投影和迭代重建)进行图像采集。每次协议扫描后,通过重新定位体模来评估可重复性,共扫描 5 次。将钙化物量化为 Agatston 评分。
将管电压降低至 100kV、剂量降低至 75%、层厚降低至 1 或 1.25mm,并结合更高的迭代重建水平,与标准的 120kV 方案相比,平均降低了 36%的扫描仪内可变性(四分位间距)。每个体模大小的扫描仪间可变性平均降低了 34%。使用标准方案,平均检测到 6.2±0.4 个钙化,而使用建议方案则检测到 7.0±0.4 个钙化。在相同体模大小的扫描仪中,Agatston 评分的两两比较显示,在标准方案中有 3 个显著不同的比较(P<0.05),而在建议方案中则没有显著不同的比较(P>0.05)。
在来自 4 家不同供应商的最先进的 CT 系统上,采用 25%的降低剂量、薄片钙评分方案可提高扫描仪内和扫描仪间的可重复性,并提高对小、低密度钙化的检测能力。在临床应用之前,该方案应进行广泛验证,但它可能会改善临床扫描仪间/机构间的可重复性,并使风险评估和治疗策略更加一致。