Fink Nicola, Zsarnoczay Emese, Schoepf U Joseph, O'Doherty Jim, Griffith Joseph P, Pinos Daniel, Tesche Christian, Ricke Jens, Willemink Martin J, Varga-Szemes Akos, Emrich Tilman
Division of Cardiovascular Imaging, Department of Radiology and Radiological Science, Medical University of South Carolina, 25 Courtenay Dr, Charleston, SC 29425, USA.
Department of Radiology, University Hospital, LMU Munich, Marchioninistr. 15, 81377 Munich, Germany.
Diagnostics (Basel). 2023 Apr 25;13(9):1540. doi: 10.3390/diagnostics13091540.
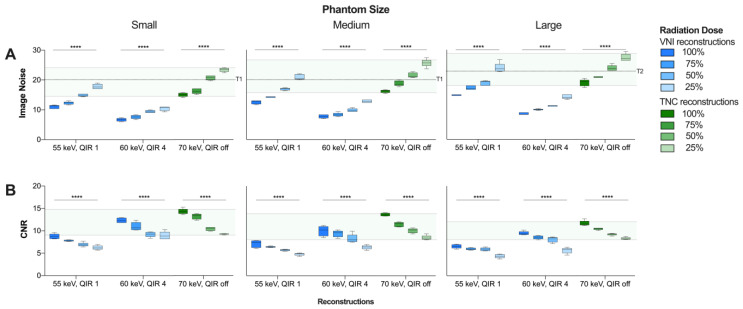
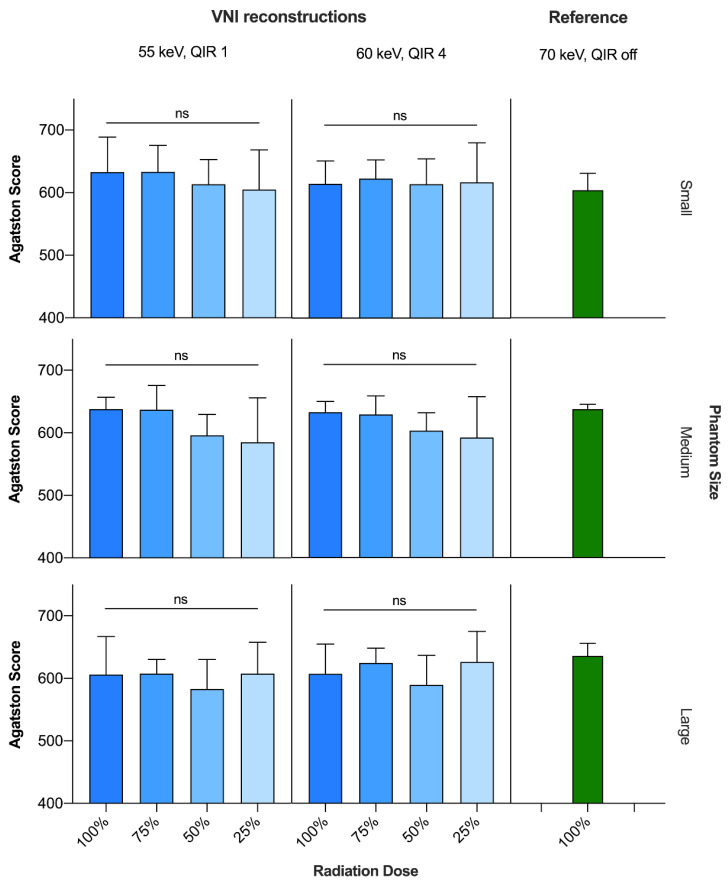
On the basis of the hypothesis that virtual noniodine (VNI)-based coronary artery calcium scoring (CACS) is feasible at reduced radiation doses, this study assesses the impact of radiation dose reduction on the accuracy of this VNI algorithm on a photon-counting detector (PCD)-CT. In a systematic in vitro setting, a phantom for CACS simulating three chest sizes was scanned on a clinical PCD-CT. The standard radiation dose was chosen at volumetric CT dose indices (CTDI) of 1.5, 3.3, 7.0 mGy for small, medium-sized, and large phantoms, and was gradually reduced by adjusting the tube current resulting in 100, 75, 50, and 25%, respectively. VNI images were reconstructed at 55 keV, quantum iterative reconstruction (QIR)1, and at 60 keV/QIR4, and evaluated regarding image quality (image noise (IN), contrast-to-noise ratio (CNR)), and CACS. All VNI results were compared to true noncontrast (TNC)-based CACS at 70 keV and standard radiation dose (reference). IN was significantly higher than IN, and IN at 55 keV/QIR1 higher than at 60 keV/QIR4 (100% dose: 16.7 ± 1.9 vs. 12.8 ± 1.7 vs. 7.7 ± 0.9; < 0.001 for every radiation dose). CNR was higher than CNR, but it was better to use 60 keV/QIR4 ( < 0.001). CACS showed strong correlation and agreement at every radiation dose ( < 0.001, r > 0.9, intraclass correlation coefficient > 0.9). The coefficients of the variation in root-mean squared error were less than 10% and thus clinically nonrelevant for the CACS of every radiation dose. This phantom study suggests that CACS is feasible on PCD-CT, even at reduced radiation dose while maintaining image quality and CACS accuracy.
基于虚拟无碘(VNI)冠状动脉钙化评分(CACS)在降低辐射剂量下可行的假设,本研究评估了辐射剂量降低对该VNI算法在光子计数探测器(PCD)CT上准确性的影响。在系统的体外环境中,在临床PCD-CT上扫描了模拟三种胸部尺寸的CACS体模。对于小、中、大尺寸体模,标准辐射剂量选择为容积CT剂量指数(CTDI)分别为1.5、3.3、7.0 mGy,并通过调整管电流逐渐降低,分别降至100%、75%、50%和25%。在55 keV、量子迭代重建(QIR)1以及60 keV/QIR4条件下重建VNI图像,并对图像质量(图像噪声(IN)、对比噪声比(CNR))和CACS进行评估。将所有VNI结果与基于70 keV和标准辐射剂量的真实非增强(TNC)CACS(参考)进行比较。IN显著高于IN,且55 keV/QIR1时的IN高于60 keV/QIR4时的IN(100%剂量:16.7±1.9 vs. 12.8±1.7 vs. 7.7±0.9;每种辐射剂量下均<0.001)。CNR高于CNR,但使用60 keV/QIR4更好(<0.001)。在每种辐射剂量下,CACS均显示出强相关性和一致性(<0.001,r>0.9,组内相关系数>0.9)。均方根误差的变异系数小于10%,因此对于每种辐射剂量的CACS在临床上不相关。该体模研究表明,即使在降低辐射剂量的情况下,CACS在PCD-CT上也是可行的,同时能保持图像质量和CACS准确性。