Laghlam Driss, Rahoual Ghilas, Malvy Julien, Estagnasié Philippe, Brusset Alain, Squara Pierre
Department of Cardiology and Critical Care, Clinique Ambroise Paré, Neuilly-sur-Seine, France.
Front Med (Lausanne). 2021 Jul 1;8:655763. doi: 10.3389/fmed.2021.655763. eCollection 2021.
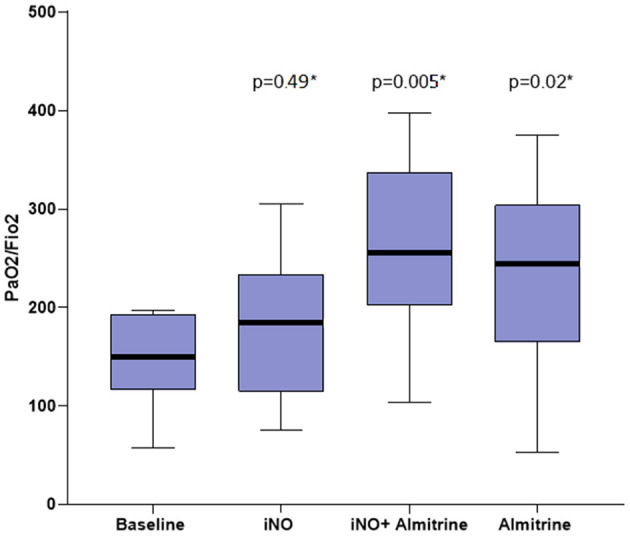
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is manifested by an acute respiratory distress syndrome (ARDS) with intense inflammation and endothelial dysfunction leading to particularly severe hypoxemia. We hypothesized that an impaired hypoxic pulmonary vasoconstriction aggravates hypoxemia. The objective of the study was to test the effect of two pulmonary vasoactive drugs on patient oxygenation. Observational, single-center, open-label study in one intensive care unit (ICU) of the Paris area, realized in April 2020. Eligible patients had coronavirus disease 2019 (COVID-19) and moderate to severe ARDS [arterial partial pressure of oxygen/fraction of inspired oxygen (PaO/FiO) <200 mmHg] despite conventional protective ventilation. Exclusion criteria included pulmonary artery hypertension defined by a pulmonary artery systolic pressure (PAPs) >45 mmHg. The assessment of oxygenation was based on PaO/FiO at (1) baseline, then after (2) 30 min of inhaled nitric oxide (iNO) 10 ppm alone, then (3) 30 min combination of iNO + almitrine infusion 8 μg/kg/min, then (4) 30 min of almitrine infusion alone. Among 20 patients requiring mechanical ventilation during the study period, 12 met the inclusion criteria. Baseline PaO/FiO was 146 ± 48 mmHg. When iNO was combined with almitrine, PaO/FiO rose to 255 ± 90 mmHg (+80 ± 49%, = 0.005), also after almitrine alone: 238 ± 98 mmHg (+67 ± 75%, = 0.02), but not after iNO alone: 185 ± 73 mmHg (+30 ± 5%, = 0.49). No adverse events related to almitrine infusion or iNO was observed. Combining iNO and infused almitrine improved the short-term oxygenation in patients with COVID-19-related ARDS. This combination may be of interest when first-line therapies fail to restore adequate oxygenation. These findings argue for an impaired pulmonary hypoxic vasoconstriction in these patients.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)表现为急性呼吸窘迫综合征(ARDS),伴有强烈炎症和内皮功能障碍,导致特别严重的低氧血症。我们推测,缺氧性肺血管收缩功能受损会加重低氧血症。本研究的目的是测试两种肺血管活性药物对患者氧合的影响。这是一项于2020年4月在巴黎地区一家重症监护病房(ICU)进行的观察性、单中心、开放标签研究。符合条件的患者患有2019冠状病毒病(COVID-19),尽管采用了传统的保护性通气,但仍患有中度至重度ARDS[动脉血氧分压/吸入氧分数(PaO/FiO)<200 mmHg]。排除标准包括肺动脉收缩压(PAPs)>45 mmHg定义的肺动脉高压。氧合评估基于以下时间点的PaO/FiO:(1)基线时,然后是(2)单独吸入10 ppm一氧化氮(iNO)30分钟后,接着是(3)iNO + 阿米三嗪以8 μg/kg/min的速度输注30分钟后,然后是(4)单独输注阿米三嗪30分钟后。在研究期间需要机械通气的20名患者中,12名符合纳入标准。基线时的PaO/FiO为146±48 mmHg。当iNO与阿米三嗪联合使用时,PaO/FiO升至255±90 mmHg(升高80±49%,P = 0.005),单独使用阿米三嗪后也有升高:238±98 mmHg(升高67±75%,P = 0.02),但单独使用iNO后无升高:185±73 mmHg(升高30±5%,P = 0.49)。未观察到与阿米三嗪输注或iNO相关的不良事件。联合使用iNO和输注阿米三嗪可改善COVID-19相关ARDS患者的短期氧合。当一线治疗未能恢复足够的氧合时,这种联合用药可能会有帮助。这些发现表明这些患者存在肺缺氧性血管收缩功能受损。