Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore.
VA Maryland Healthcare System, Baltimore.
JAMA Netw Open. 2021 Jul 1;4(7):e2119747. doi: 10.1001/jamanetworkopen.2021.19747.
Knowing the expected effect of treatment on an individual patient is essential for patient care.
To explore clinicians' conceptualizations of the chance that treatments will decrease the risk of disease outcomes.
DESIGN, SETTING, AND PARTICIPANTS: This survey study of attending and resident physicians, nurse practitioners, and physician assistants was conducted in outpatient clinical settings in 8 US states from June 2018 to November 2019. The survey was an in-person, paper, 26-item survey in which clinicians were asked to estimate the probability of adverse disease outcomes and expected effects of therapies for diseases common in primary care.
Estimated chance that treatments would benefit an individual patient.
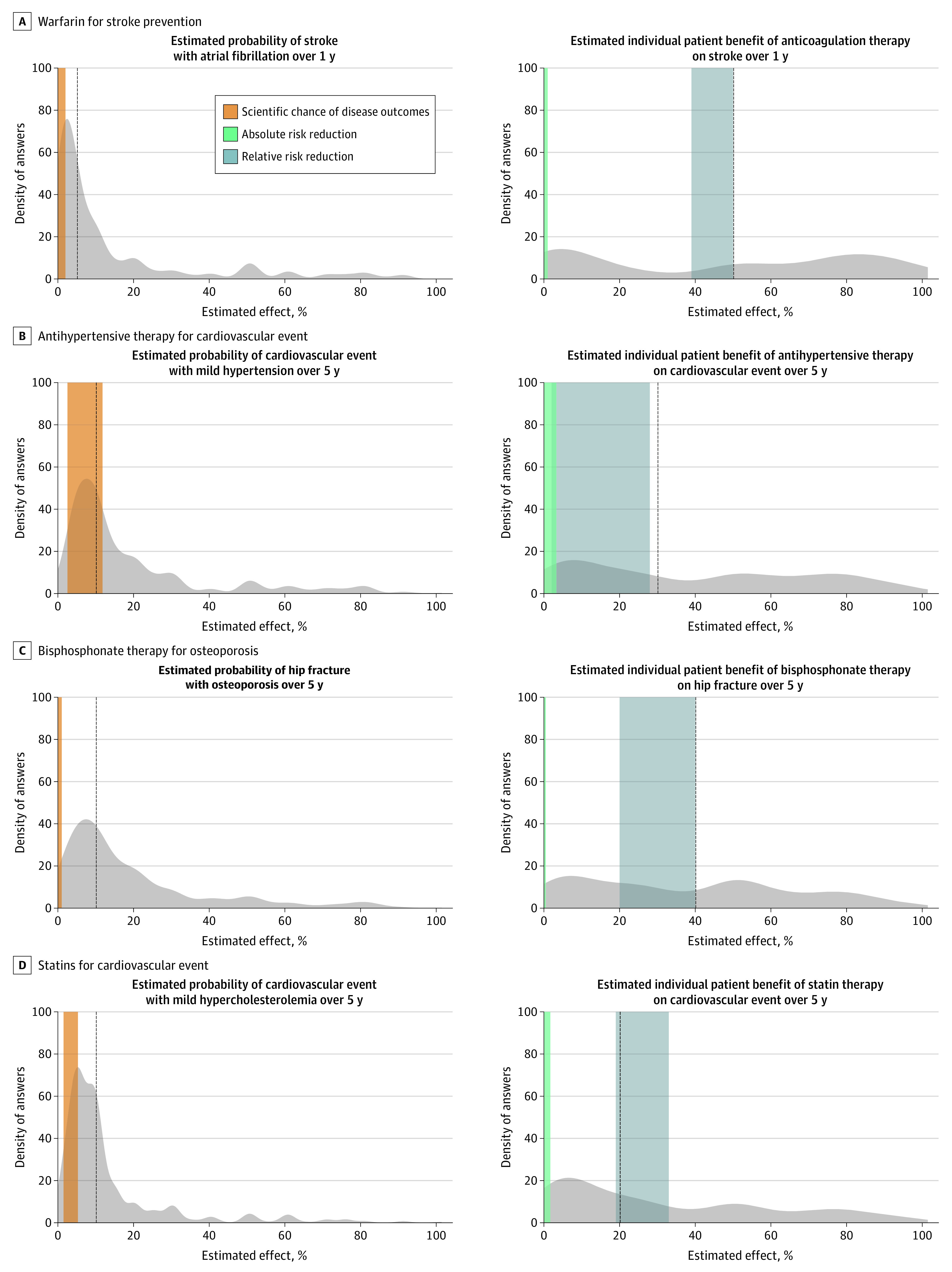
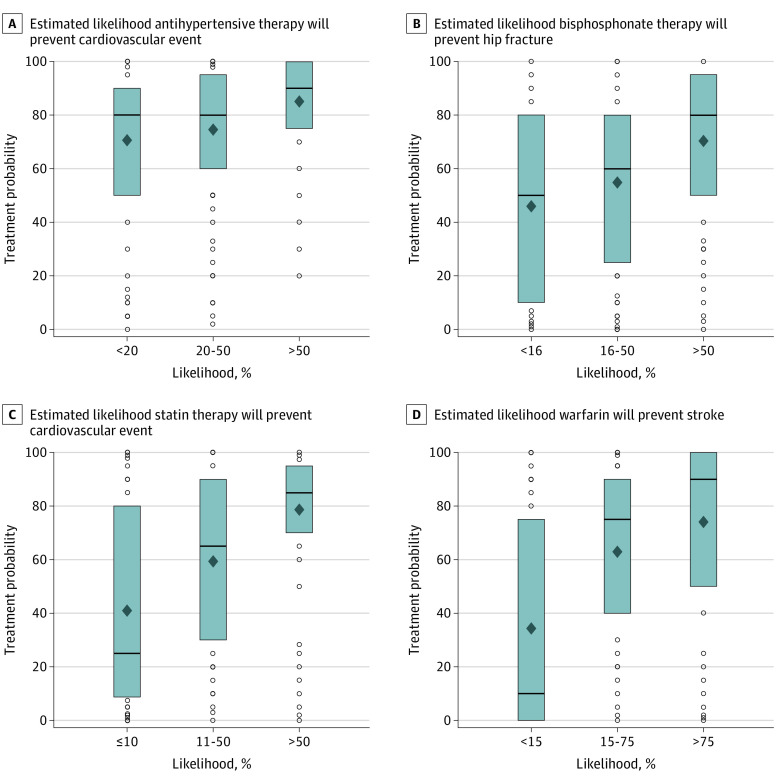
Of 723 clinicians, 585 (81%) responded, and 542 completed all the questions necessary for analysis, with a median (interquartile range [IQR]) age of 32 (29-44) years, 287 (53%) women, and 294 (54%) White participants. Clinicians consistently overestimated the chance that treatments would benefit an individual patient. The median (IQR) estimated chance that warfarin would prevent a stroke in the next year was 50% (5%-80%) compared with scientific evidence, which indicates an absolute risk reduction (ARR) of 0.2% to 1.0% based on a relative risk reduction (RRR) of 39% to 50%. The median (IQR) estimated chance that antihypertensive therapy would prevent a cardiovascular event within 5 years was 30% (10%-70%) vs evidence of an ARR of 0% to 3% based on an RRR of 0% to 28%. The median (IQR) estimated chance that bisphosphonate therapy would prevent a hip fracture in the next 5 years was 40% (10%-60%) vs evidence of ARR of 0.1% to 0.4% based on an RRR of 20% to 40%. The median (IQR) estimated chance that moderate-intensity statin therapy would prevent a cardiovascular event in the next 5 years was 20% (IQR 5%-50%) vs evidence of an ARR of 0.3% to 2% based on an RRR of 19% to 33%. Estimates of the chance that a treatment would prevent an adverse outcome exceeded estimates of the absolute chance of that outcome for 60% to 70% of clinicians. Clinicians whose overestimations were greater were more likely to report using that treatment for patients in their practice (eg, use of warfarin: correlation coefficient, 0.46; 95% CI, 0.40-0.53; P < .001).
In this survey study, clinicians significantly overestimated the benefits of treatment to individual patients. Clinicians with greater overestimates were more likely to report using treatments in actual patients.
了解治疗对个体患者的预期效果对于患者护理至关重要。
探索临床医生对治疗降低疾病结局风险的可能性的概念理解。
设计、地点和参与者:这项在 8 个美国州的门诊临床环境中进行的调查研究,调查对象为主治医生和住院医生、执业护士和医师助理。调查是一项现场纸质的 26 项调查,要求临床医生估计不良疾病结果的概率和常见于初级保健的疾病治疗效果。
治疗对个体患者有益的估计概率。
在 723 名临床医生中,有 585 名(81%)做出了回应,其中 542 名完成了所有必要的分析问题,中位数(四分位距 [IQR])年龄为 32(29-44)岁,287 名(53%)为女性,294 名(54%)为白人参与者。临床医生一直高估了治疗对个体患者有益的概率。华法林在接下来一年预防中风的估计概率中位数(IQR)为 50%(5%-80%),而科学证据表明,基于相对风险降低(RRR)39%-50%,绝对风险降低(ARR)为 0.2%-1.0%。降压治疗在 5 年内预防心血管事件的估计概率中位数(IQR)为 30%(10%-70%),而证据表明基于 RRR 0%-28%,ARR 为 0%-3%。双膦酸盐治疗在接下来 5 年内预防髋部骨折的估计概率中位数(IQR)为 40%(10%-60%),而证据表明基于 RRR 20%-40%,ARR 为 0.1%-0.4%。中等强度他汀类药物治疗在接下来 5 年内预防心血管事件的估计概率中位数(IQR)为 20%(5%-50%),而证据表明基于 RRR 19%-33%,ARR 为 0.3%-2%。治疗预防不良结果的概率估计值超过了 60%-70%的临床医生对该结果的绝对概率的估计值。对治疗的益处高估更大的临床医生更有可能在实际患者中报告使用该治疗方法(例如,使用华法林:相关系数为 0.46;95%置信区间,0.40-0.53;P < 0.001)。
在这项调查研究中,临床医生显著高估了治疗对个体患者的益处。对治疗效果高估更大的临床医生更有可能在实际患者中报告使用该治疗方法。