Department of Public Health, Pwani University, P.O Box 195, Kilifi, 80108, Kenya.
KEMRI/Wellcome Trust Research Programme, P.O Box 230, Kilifi, 80108, Kenya.
Sci Rep. 2021 Jul 21;11(1):14854. doi: 10.1038/s41598-021-94153-0.
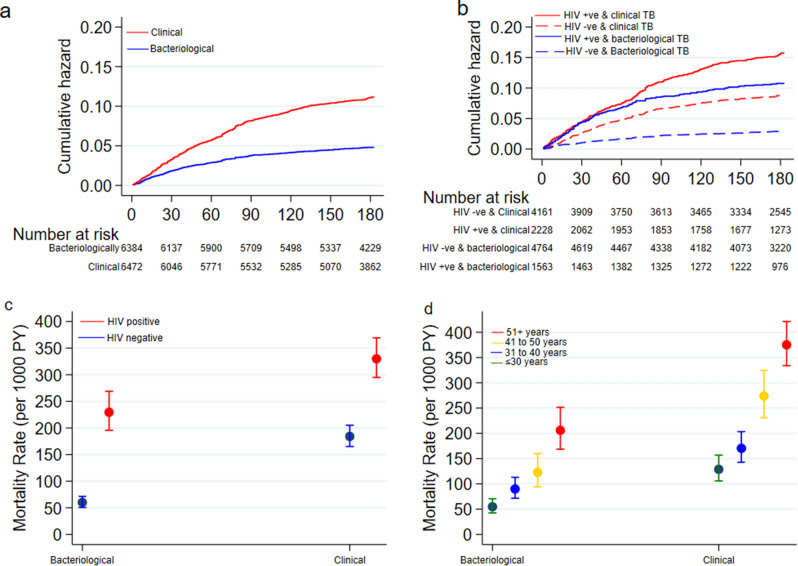
The World Health Organization (WHO) criteria for diagnosing and treating Tuberculosis (TB) includes clinical signs, therefore not requiring bacteriological laboratory confirmation. In resource-limited settings, including Kenya, this empirical TB treatment is routine practice however limited data exist on patient clinical outcomes when comparing the method of diagnosis. We evaluated TB treatment outcomes comparing clinically diagnosed and bacteriologically confirmed TB, 6 months after starting treatment of TB in a rural county in Kenya. Our analysis compared patients with a clinical versus a bacteriologically confirmed TB diagnosis. In this retrospective analysis, we included all adults (≥ 18 years) starting treatment of TB and followed up for 6 months, within the County TB surveillance database from 2012 to 2018. Patients included from both public and private facilities. The TB treatment outcomes assessed included treatment success, treatment failure, death, defaulted and transferred out. We used survival regression models to assess effect of type of diagnosis on TB treatment outcome defining time at risk from date of starting treatment to experiencing one of the treatment outcomes or completing 6-months of treatment. A total of 12,856 patients; median age 37 [IQR 28 - 50] years were included. 7639 (59%) were male while 11,339 (88%) were pulmonary TB cases. Overall, 11,633 (90%) were given first-line TB treatment and 3791 (29%) were HIV infected. 6472 (50%) of the patients were clinically diagnosed of whom 4521/6472 (70%) had a negative sputum/GeneXpert test. During the study 5565 person-years (PYs) observed, treatment success was 82% and 83% amongst clinically and bacteriologically diagnosed patients (P = 0.05). There were no significant differences in defaulting (P = 0.70) or transfer out (P = 0.19) between clinically and bacteriologically diagnosed patients. Mortality was significantly higher among clinically diagnosed patients: 639 (9.9%) deaths compared to 285 (4.5%) amongst the bacteriologically diagnosed patients; aHR 5.16 (95%CI 2.17 - 12.3) P < 0.001. Our study suggests survival during empirical TB treatment is significantly lower compared to patients with laboratory evidence, irrespective of HIV status and age. To improve TB treatment outcomes amongst clinically diagnosed patients, we recommend systematic screening for comorbidities, prompt diagnosis and management of other infections.
世界卫生组织(WHO)诊断和治疗结核病(TB)的标准包括临床症状,因此不需要细菌学实验室确认。在资源有限的环境中,包括肯尼亚,这种经验性结核病治疗是常规做法,但在比较诊断方法时,关于患者临床结果的数据有限。我们评估了在肯尼亚农村县开始治疗结核病 6 个月后,比较临床诊断和细菌学确诊结核病的结核病治疗结果。我们的分析比较了具有临床诊断和细菌学确诊结核病的患者。在这项回顾性分析中,我们纳入了 2012 年至 2018 年期间,县结核病监测数据库中所有开始接受结核病治疗并随访 6 个月的成年人(≥18 岁)。患者包括来自公共和私人设施的患者。评估的结核病治疗结果包括治疗成功、治疗失败、死亡、失访和转院。我们使用生存回归模型来评估诊断类型对结核病治疗结果的影响,将风险时间定义为从开始治疗之日起至出现治疗结果之一或完成 6 个月治疗的时间。共纳入 12856 例患者;中位年龄 37 [IQR 28-50] 岁。7639 例(59%)为男性,11339 例(88%)为肺结核病例。总体而言,11633 例(90%)接受一线结核病治疗,3791 例(29%)感染了 HIV。6472 例(50%)患者经临床诊断,其中 4521/6472 例(70%)痰/基因 Xpert 检测阴性。在研究期间观察到 5565 人年(PY),临床和细菌学诊断患者的治疗成功率分别为 82%和 83%(P=0.05)。临床和细菌学诊断患者的失访率(P=0.70)或转院率(P=0.19)无显著差异。临床诊断患者的死亡率明显更高:639 例(9.9%)死亡,而细菌学诊断患者 285 例(4.5%);aHR 5.16(95%CI 2.17-12.3)P<0.001。我们的研究表明,与具有实验室证据的患者相比,经验性结核病治疗期间的生存率显著降低,无论 HIV 状态和年龄如何。为了提高临床诊断患者的结核病治疗结果,我们建议系统筛查合并症,及时诊断和治疗其他感染。