Aries Alison M, Pomeroy Valerie M, Sim Julius, Read Susan, Hunter Susan M
School of Allied Health Professions, Faculty of Medicine and Health Sciences, Keele University, Keele, United Kingdom.
Acquired Brain Injury Recovery Alliance (ABIRA), School of Health Sciences, University of East Anglia, Norwich, United Kingdom.
Front Neurol. 2021 Jul 5;12:675106. doi: 10.3389/fneur.2021.675106. eCollection 2021.
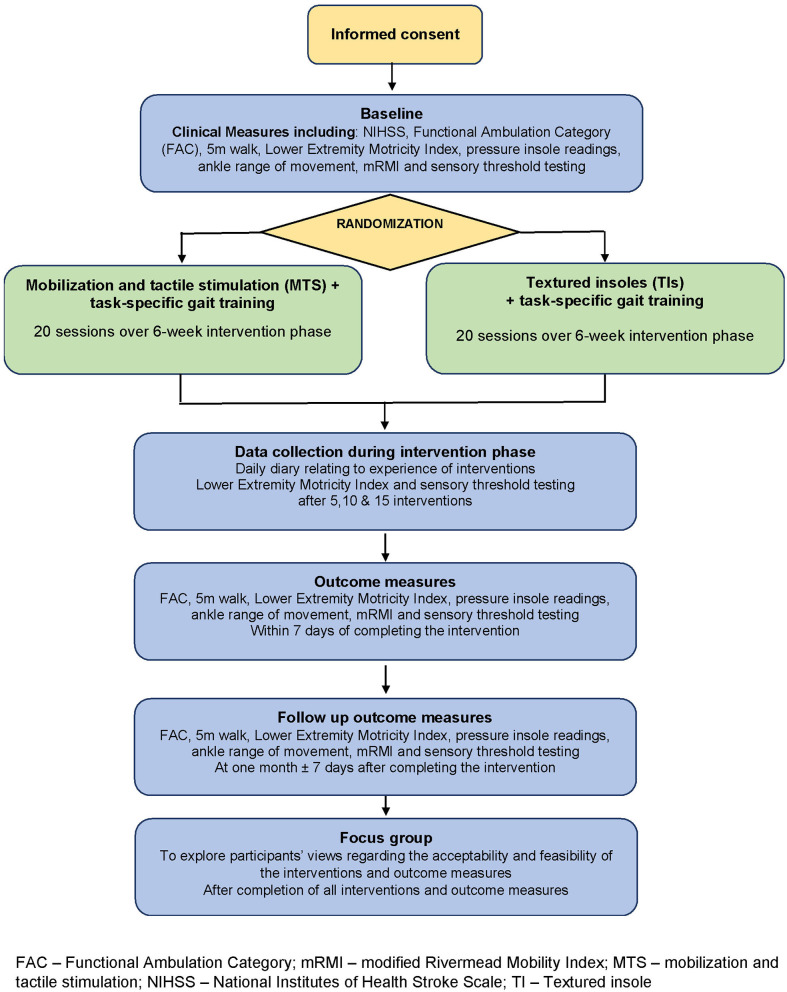
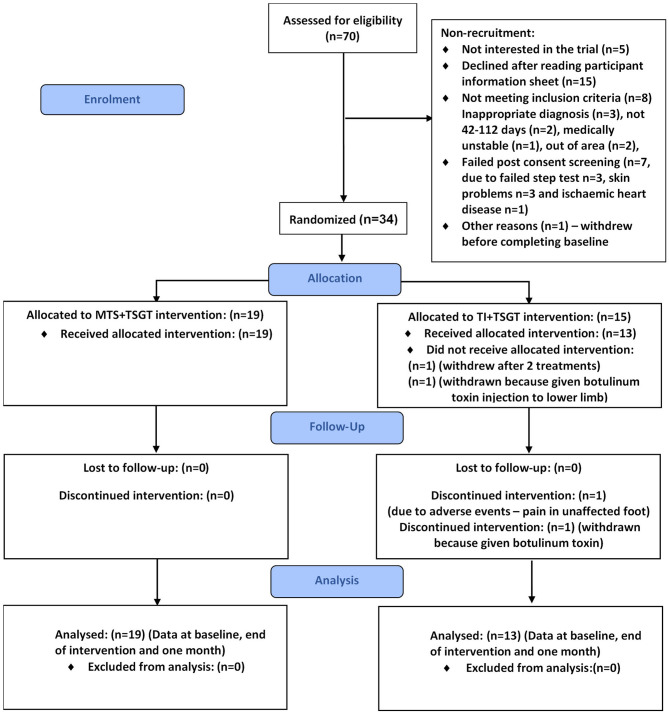
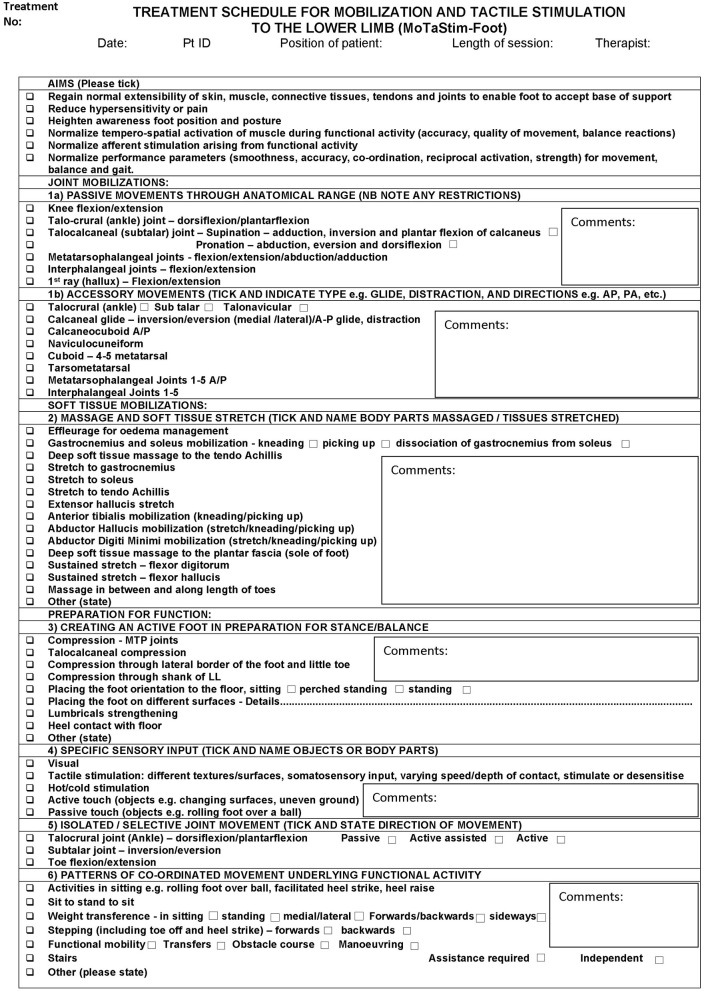
Somatosensory stimulation of the lower extremity could improve motor recovery and walking post-stroke. This pilot study investigated the feasibility of a subsequent randomized controlled trial (RCT) to determine whether task-specific gait training is more effective following either (a) intensive hands-on somatosensory stimulation or (b) wearing textured insoles. Determine recruitment and attrition rates, adherence to intervention, acceptability and viability of interventions and outcome measures, and estimate variance of outcome data to inform sample size for a subsequent RCT. Design: randomized, single-blinded, mixed-methods pilot study. In-patient rehabilitation ward and community. = 34, 18+years, 42-112 days following anterior or posterior circulation stroke, able to follow simple commands, able to walk independently pre-stroke, and providing informed consent. Twenty 30-min sessions of task-specific gait training (TSGT) (delivered over 6 weeks) in addition to either: (a) 30-60 min mobilization and tactile stimulation (MTS); or (b) unlimited textured insole (TI) wearing. Ankle range of movement (electrogoniometer), touch-pressure sensory thresholds (Semmes Weinstein Monofilaments), motor impairment (Lower Extremity Motricity Index), walking ability and speed (Functional Ambulation Category, 5-m walk test, pressure insoles) and function (modified Rivermead Mobility Index), measured before randomization, post-intervention, and 1-month thereafter (follow-up). Adherence to allocated intervention and actual dose delivered (fidelity) were documented in case report forms and daily diaries. Focus groups further explored acceptability of interventions and study experience. Recruitment, attrition, and dose adherence rates were calculated as percentages of possible totals. Thematic analysis of daily diaries and focus group data was undertaken. Standard deviations of outcome measures were calculated and used to inform a sample size calculation. Recruitment, attrition, and adherence rates were 48.57, 5.88, and 96.88%, respectively. Focus groups, daily-diaries and case report forms indicated acceptability of interventions and outcome measures to participants. The 5-m walk was selected as primary outcome measure for a future trial [mean (SD) at end of intervention: 16.86 (11.24) MTS group and 21.56 (13.57) TI group]; sample size calculation indicated 60 participants are required per group. Recruitment, attrition and adherence rates and acceptability of interventions and outcomes justify a subsequent powered RCT of MTS+TSGT compared with TI+TSGT.
对下肢进行体感刺激可改善中风后的运动恢复和步行能力。这项初步研究调查了后续随机对照试验(RCT)的可行性,以确定在以下两种情况后,特定任务步态训练是否更有效:(a)强化的亲身体感刺激;或(b)穿着有纹理的鞋垫。确定招募率和损耗率、对干预措施的依从性、干预措施和结果测量的可接受性和可行性,并估计结果数据的方差,以为后续RCT提供样本量信息。设计:随机、单盲、混合方法的初步研究。住院康复病房和社区。n = 34,年龄18岁及以上,在前循环或后循环中风后42 - 112天,能够听从简单指令,中风前能够独立行走,并提供知情同意书。除了以下两种情况之一外,进行20次30分钟的特定任务步态训练(TSGT)(在6周内完成):(a)30 - 60分钟的活动和触觉刺激(MTS);或(b)不限时长地穿着有纹理的鞋垫(TI)。在随机分组前、干预后以及此后1个月(随访)测量踝关节活动范围(电子角度计)、触觉压力感觉阈值(Semmes Weinstein单丝)、运动障碍(下肢运动指数)、步行能力和速度(功能性步行分类、5米步行测试、压力鞋垫)以及功能(改良的Rivermead活动指数)。在病例报告表和每日日记中记录对分配干预措施的依从性和实际给予的剂量(保真度)。焦点小组进一步探讨了干预措施的可接受性和研究体验。招募率、损耗率和剂量依从率以可能总数的百分比计算。对每日日记和焦点小组数据进行主题分析。计算结果测量的标准差并用于样本量计算。招募率、损耗率和依从率分别为48.57%、5.88%和96.88%。焦点小组、每日日记和病例报告表表明参与者对干预措施和结果测量具有可接受性。选择5米步行作为未来试验的主要结果测量指标[干预结束时的均值(标准差):MTS组为16.86(11.24),TI组为21.56(13.57)];样本量计算表明每组需要60名参与者。招募率、损耗率和依从率以及干预措施和结果的可接受性证明了随后进行的MTS + TSGT与TI + TSGT的有足够效力的RCT是合理的。