Oral and Maxillofacial Surgery Department, King's College Hospital NHS Foundation Trust, Denmark Hill, SE1 9RT London, United Kingdom.
Liver Intensive Care Unit, Department of Critical Care, King's College Hospital NHS Foundation Trust, Denmark Hill, SE1 9RT London, United Kingdom.
Br J Oral Maxillofac Surg. 2021 Nov;59(9):1013-1023. doi: 10.1016/j.bjoms.2021.05.011. Epub 2021 May 18.
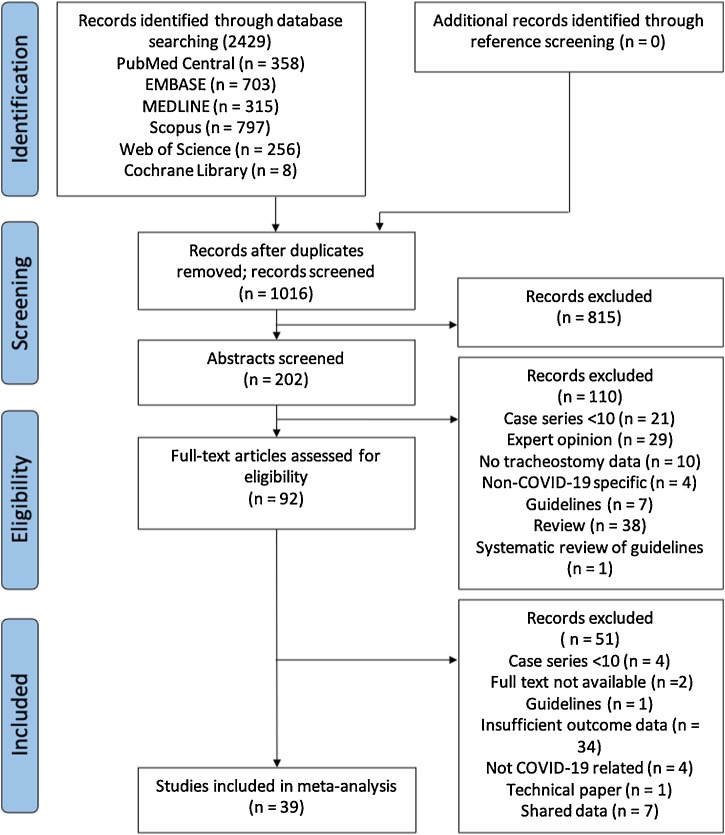
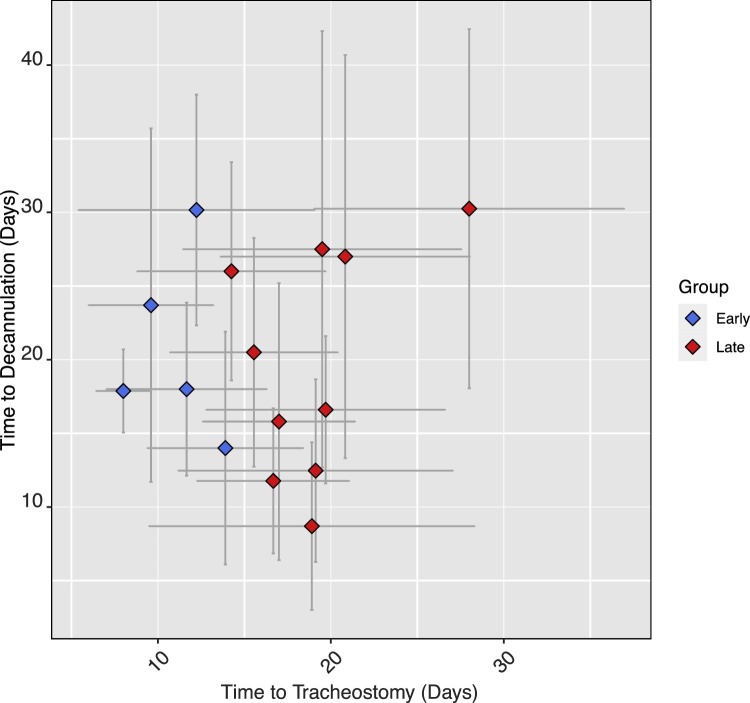
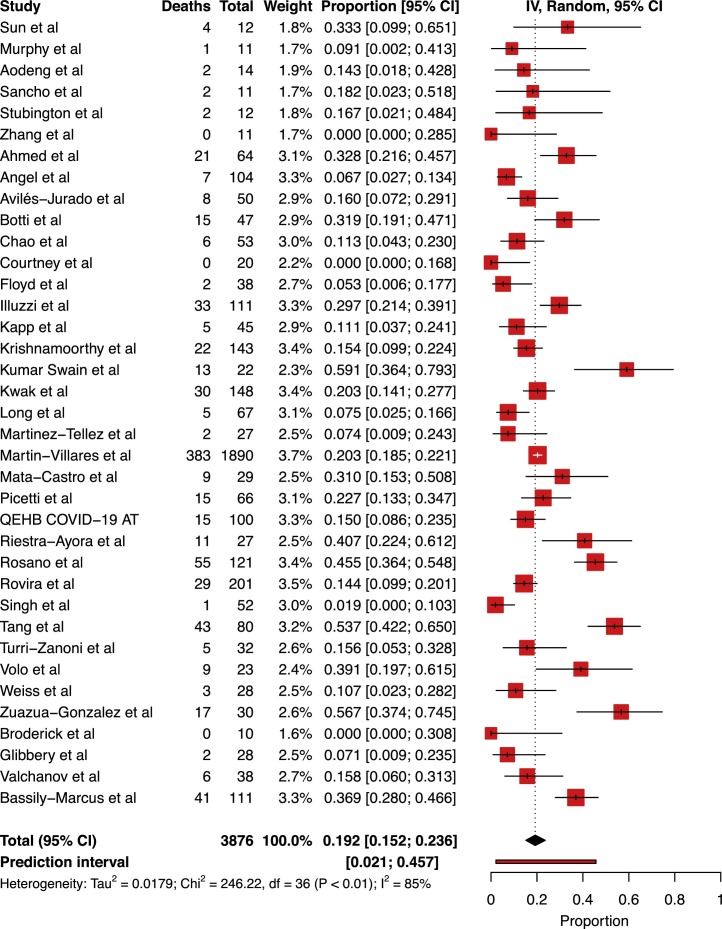
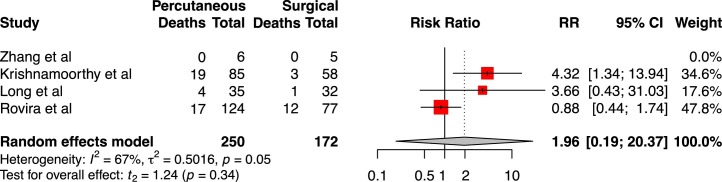
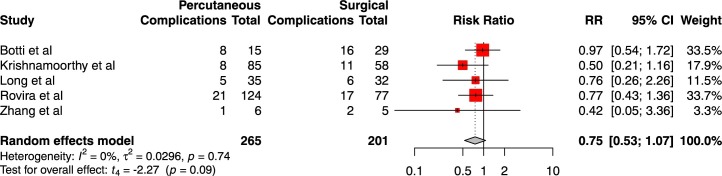
A systematic review and meta-analysis of the entire COVID-19 Tracheostomy cohort was conducted to determine the cumulative incidence of complications, mortality, time to decannulation and ventilatory weaning. Outcomes of surgical versus percutaneous and outcomes relative to tracheostomy timing were also analysed. Studies reporting outcome data on patients with COVID-19 undergoing tracheostomy were identified and screened by 2 independent reviewers. Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed. Outcome data were analysed using a random-effects model. From 1016 unique studies, 39 articles reporting outcomes for a total of 3929 patients were included for meta-analysis. Weighted mean follow-up time was 42.03±26 days post-tracheostomy. Meta-analysis showed that 61.2% of patients were weaned from mechanical ventilation [95%CI 52.6%-69.5%], 44.2% of patients were decannulated [95%CI 33.96%-54.67%], and cumulative mortality was found to be 19.23% [95%CI 15.2%-23.6%] across the entire tracheostomy cohort. The cumulative incidence of complications was 14.24% [95%CI 9.6%-19.6%], with bleeding accounting for 52% of all complications. No difference was found in incidence of mortality (RR1.96; p=0.34), decannulation (RR1.35, p=0.27), complications (RR0.75, p=0.09) and time to decannulation (SMD 0.46, p=0.68) between percutaneous and surgical tracheostomy. Moreover, no difference was found in mortality (RR1.57, p=0.43) between early and late tracheostomy, and timing of tracheostomy did not predict time to decannulation. Ten confirmed nosocomial staff infections were reported from 1398 tracheostomies. This study provides an overview of outcomes of tracheostomy in COVID-19 patients, and contributes to our understanding of tracheostomy decisions in this patient cohort.
对整个 COVID-19 气管切开术队列进行了系统回顾和荟萃分析,以确定并发症的累积发生率、死亡率、拔管时间和通气脱机时间。还分析了手术与经皮和相对于气管切开术时机的结果。通过 2 名独立审查员确定并筛选了报告 COVID-19 患者接受气管切开术的结果数据的研究。遵循系统评价和荟萃分析的首选报告项目 (PRISMA) 指南。使用随机效应模型分析结果数据。从 1016 项独特的研究中,有 39 篇文章报告了总共 3929 名患者的结果,被纳入荟萃分析。加权平均随访时间为气管切开术后 42.03±26 天。荟萃分析显示,61.2%的患者成功脱机[95%CI 52.6%-69.5%],44.2%的患者拔管[95%CI 33.96%-54.67%],整个气管切开术队列的累积死亡率为 19.23%[95%CI 15.2%-23.6%]。并发症的累积发生率为 14.24%[95%CI 9.6%-19.6%],出血占所有并发症的 52%。经皮与手术气管切开术之间在死亡率(RR1.96;p=0.34)、拔管(RR1.35,p=0.27)、并发症(RR0.75,p=0.09)和拔管时间(SMD 0.46,p=0.68)方面无差异。此外,早期和晚期气管切开术之间的死亡率无差异(RR1.57,p=0.43),气管切开术的时机并不能预测拔管时间。从 1398 例气管切开术中共报告了 10 例确诊的医院工作人员感染。本研究概述了 COVID-19 患者气管切开术的结果,并有助于我们了解该患者群体中气管切开术的决策。