Kuo Chien-Yi, Lin Chieh-Hsin, Lane Hsien-Yuan
Department of Psychiatry, China Medical University Hospital, Taichung 40402, Taiwan.
Graduate Institute of Biomedical Sciences, China Medical University, Taichung 40402, Taiwan.
Int J Mol Sci. 2021 Jul 10;22(14):7421. doi: 10.3390/ijms22147421.
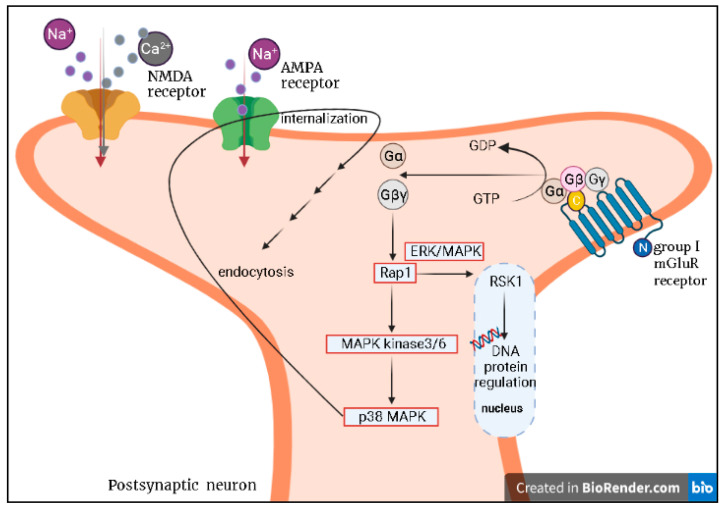
Late-life depression (LLD), compared to depression at a young age, is more likely to have poor prognosis and high risk of progression to dementia. A recent systemic review and meta-analysis of the present antidepressants for LLD showed that the treatment response rate was 48% and the remission rate was only 33.7%, thus implying the need to improve the treatment with other approaches in the future. Recently, agents modulating the glutamatergic system have been tested for mental disorders such as schizophrenia, dementia, and depressive disorder. Ketamine, a noncompetitive NMDA receptor (NMDAR) antagonist, requires more evidence from randomized clinical trials (RCTs) to prove its efficacy and safety in treating LLD. The metabotropic receptors (mGluRs) of the glutamatergic system are family G-protein-coupled receptors, and inhibition of the Group II mGluRs subtypes (mGlu2 and mGlu3) was found to be as effective as ketamine in exerting rapid antidepressant activity in some animal studies. Inflammation has been thought to contribute to depression for a long time. The cytokine levels not only increase with age but also decrease serotonin. Regarding LLD, interleukin 6 (IL-6) and tumor necrosis factor α (TNF-α) released in vivo are likely to contribute to the reduced serotonin level. Brain-derived neurotrophic factor (BDNF), a growth factor and a modulator in the tropomyosin receptor kinase (Trk) family of tyrosine kinase receptors, probably declines quantitatively with age. Recent studies suggest that BDNF/TrkB decrement may contribute to learning deficits and memory impairment. In the process of aging, physiological changes in combination with geriatric diseases such as vascular diseases result in poorer prognosis of LLD in comparison with that of young-age depression. Treatments with present antidepressants have been generally unsatisfactory. Novel treatments such as anti-inflammatory agents or NMDAR agonists/antagonists require more studies in LLD. Last but not least, LLD and dementia, which share common pathways and interrelate reciprocally, are a great concern. If it is possible to enhance the treatment of LDD, dementia can be prevented or delated.
与年轻时的抑郁症相比,老年期抑郁症(LLD)更有可能预后不良,且发展为痴呆症的风险较高。最近一项针对目前用于治疗LLD的抗抑郁药的系统评价和荟萃分析表明,治疗有效率为48%,缓解率仅为33.7%,这意味着未来需要采用其他方法来改善治疗效果。最近,调节谷氨酸能系统的药物已在精神疾病如精神分裂症、痴呆症和抑郁症中进行了测试。氯胺酮是一种非竞争性N-甲基-D-天冬氨酸受体(NMDAR)拮抗剂,需要更多随机临床试验(RCT)的证据来证明其治疗LLD的有效性和安全性。谷氨酸能系统的代谢型受体(mGluRs)是G蛋白偶联受体家族,在一些动物研究中发现,抑制II组mGluRs亚型(mGlu2和mGlu3)在发挥快速抗抑郁活性方面与氯胺酮一样有效。长期以来,炎症一直被认为与抑郁症有关。细胞因子水平不仅随年龄增长而升高,还会降低血清素水平。对于LLD,体内释放的白细胞介素6(IL-6)和肿瘤坏死因子α(TNF-α)可能导致血清素水平降低。脑源性神经营养因子(BDNF)是一种生长因子,也是酪氨酸激酶受体原肌球蛋白受体激酶(Trk)家族中的调节剂,其含量可能会随着年龄的增长而定量下降。最近的研究表明,BDNF/TrkB的减少可能导致学习缺陷和记忆障碍。在衰老过程中,生理变化与老年疾病(如血管疾病)相结合,导致LLD的预后比年轻时的抑郁症更差。目前使用抗抑郁药进行治疗普遍效果不佳。抗炎药或NMDAR激动剂/拮抗剂等新疗法在LLD方面需要更多研究。最后但同样重要的是,LLD和痴呆症有着共同的途径且相互关联,这是一个重大问题。如果能够加强对LLD的治疗,就可以预防或延缓痴呆症的发生。