From the Department of Physical Medicine and Rehabilitation, Rutgers New Jersey Medical School, Newark, NJ; Rutgers New Jersey Medical School, Newark, NJ; Kessler Institute for Rehabilitation, West Orange, NJ.
Rutgers New Jersey Medical School, Newark, NJ.
Arch Phys Med Rehabil. 2021 Dec;102(12):2291-2299. doi: 10.1016/j.apmr.2021.07.003. Epub 2021 Jul 23.
To measure discharge disposition, length of stay (LOS), and functional activities of daily living (ADL) scores for patients admitted to acute inpatient rehabilitation hospitals (IRHs) during the coronavirus disease 2019 (COVID-19) pandemic and to compare these parameters with a period prior to the pandemic.
Retrospective cohort study via systematic retrospective chart review of consecutive patients admitted to IRHs from January 1-February 19, 2020 (pre-COVID-19T), and COVID-19 time period/patients admitted from April 1, 2020-May 9, 2020 (COVID-19T).
System of 3 IRHs in the Northeastern United States.
Pre-COVID-19T, n=739; COVID-19T, n=335, of whom n=139 were positive for COVID-19 (COVID+) and n=196 were negative (COVID-) (N=1074).
Not applicable.
Discharge disposition, LOS, and functional ADL scores.
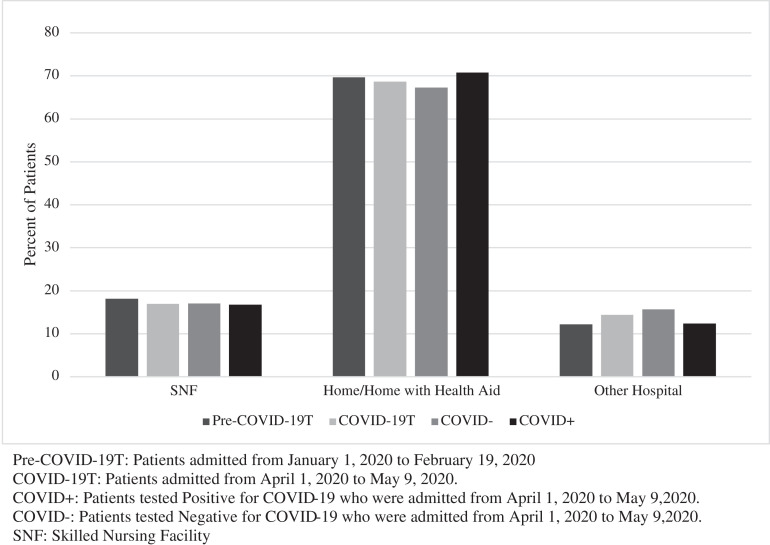
COVID-19T patients were younger (P=.03) and less likely to be White (P=.03). These patients also had a higher case mix index (CMI; P<.01), longer acute care LOS (P<.01), and longer IRH LOS (P<.01). Patients who were COVID+ (during COVID-19T) were less likely to be White (P<.01), had lower CMI (P<.01), had higher admission and discharge functional ADL scores (P=.02, P<.01), and had longer acute care LOS compared with those who were COVID- (P<.01). There were no differences in discharge outcomes between pre-COVID-19T and COVID-19T cohorts (P=.75), including when stratified for COVID-19 status (P=.74). Functional ADL scores on admission and discharge were lower in COVID-19T than in pre-COVID-19T (P=.01), including when stratified for COVID-19 status though not significant (P=.06).
There were no differences in discharge outcomes for any group. IRH LOS was significantly increased during the pandemic, but there were no statistically significant differences between the COVID+ and COVID- cohorts within COVID-19T. Functional ADL scores were significantly lower during COVID-19T, but COVID status was not a significant predictor. This suggests that COVID+ status was not a barrier to discharge or functional outcomes. This supports the importance of IRHs to restore function and discharge patients to home, even with a more medically complex COVID-19 pandemic population.
测量在 2019 年冠状病毒病(COVID-19)大流行期间入住急性住院康复医院(IRH)的患者的出院情况、住院时间(LOS)和日常生活活动(ADL)功能评分,并将这些参数与大流行前的时期进行比较。
通过对 2020 年 1 月 1 日至 2 月 19 日(COVID-19T 前)和 COVID-19 期间/2020 年 4 月 1 日至 5 月 9 日期间(COVID-19T)连续入住 IRH 的患者进行系统回顾性图表回顾的回顾性队列研究。
美国东北部的 3 个 IRH 系统。
COVID-19T 前组,n=739;COVID-19T 组,n=335,其中 n=139 例 COVID-19 阳性(COVID+),n=196 例 COVID-19 阴性(COVID-)(n=1074)。
不适用。
出院情况、住院时间和功能 ADL 评分。
COVID-19T 患者年龄更小(P=.03),且白人比例更低(P=.03)。这些患者的病例组合指数(CMI;P<.01)更高,急性护理 LOS 更长(P<.01),IRH LOS 也更长(P<.01)。与 COVID- 患者相比,COVID+(在 COVID-19T 期间)患者的白人比例更低(P<.01),CMI 更低(P<.01),入院和出院时的 ADL 功能评分更高(P=.02,P<.01),且急性护理 LOS 也更长(P<.01)。COVID-19T 前和 COVID-19T 队列之间在出院结果方面没有差异(P=.75),包括 COVID-19 状态分层时(P=.74)。COVID-19T 患者的入院和出院时的 ADL 功能评分均低于 COVID-19T 前(P=.01),尽管没有统计学意义(P=.06),但 COVID-19 状态分层时并非如此。
任何组之间的出院结果均无差异。大流行期间 IRH 的 LOS 显著增加,但 COVID-19T 内 COVID+和 COVID-队列之间没有统计学上的显著差异。COVID-19T 期间的 ADL 功能评分明显降低,但 COVID 状态不是显著的预测因素。这表明 COVID+状态不是出院或功能结果的障碍。这支持了 IRH 对于恢复功能和将患者出院回家的重要性,即使面对更具医学复杂性的 COVID-19 大流行人群也是如此。