National Institute for Health Research Health Protection Research Unit in Emerging and Zoonotic Infections, Institute of Infection, Veterinary and Ecological Sciences, University of Liverpool, Liverpool, UK; The Walton Centre National Health Service (NHS) Foundation Trust, Liverpool, UK.
Queen Square Institute of Neurology, University College London, London, UK.
Lancet Neurol. 2020 Sep;19(9):767-783. doi: 10.1016/S1474-4422(20)30221-0. Epub 2020 Jul 2.
The COVID-19 pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is of a scale not seen since the 1918 influenza pandemic. Although the predominant clinical presentation is with respiratory disease, neurological manifestations are being recognised increasingly. On the basis of knowledge of other coronaviruses, especially those that caused the severe acute respiratory syndrome and Middle East respiratory syndrome epidemics, cases of CNS and peripheral nervous system disease caused by SARS-CoV-2 might be expected to be rare.
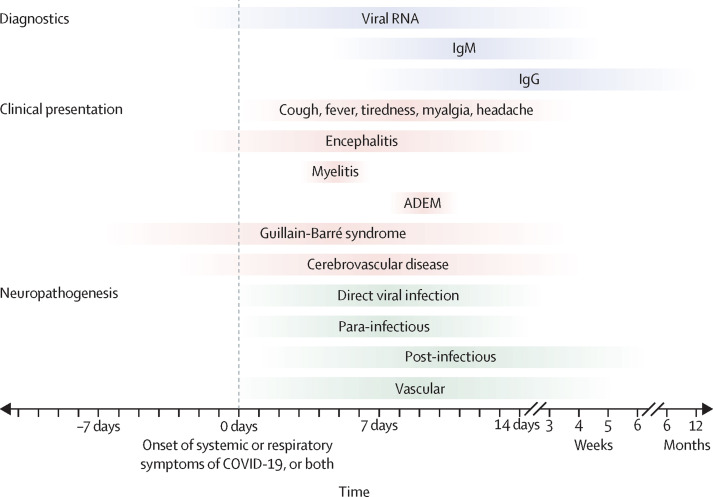
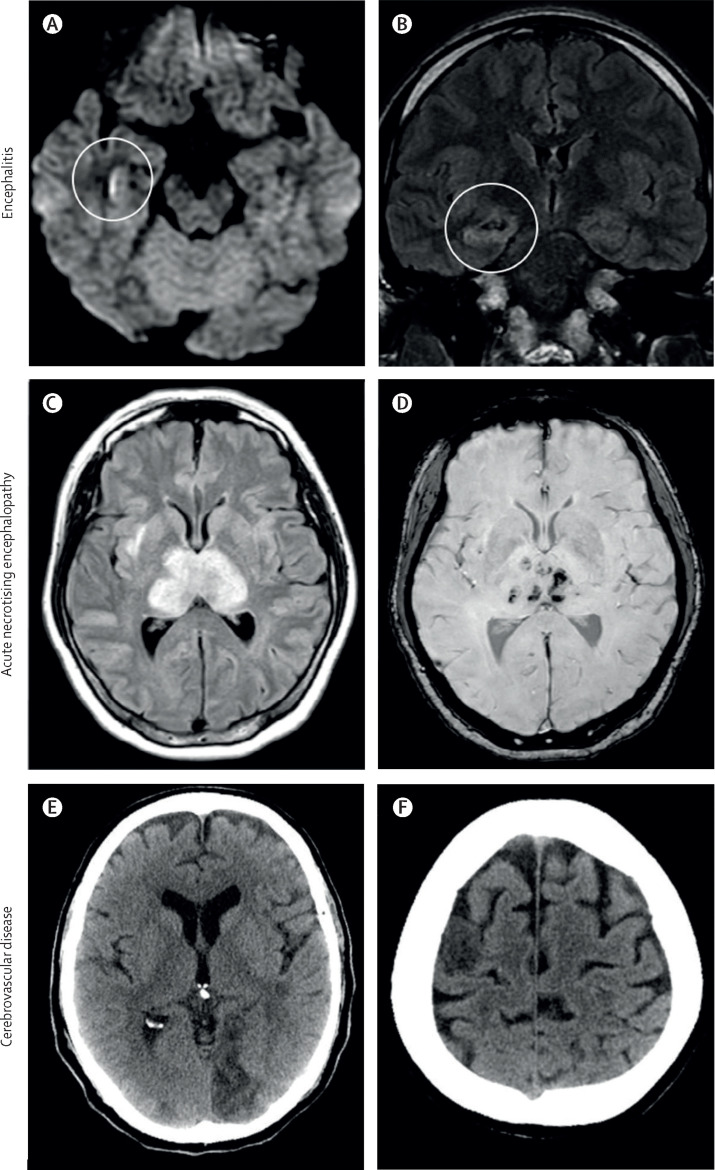
A growing number of case reports and series describe a wide array of neurological manifestations in 901 patients, but many have insufficient detail, reflecting the challenge of studying such patients. Encephalopathy has been reported for 93 patients in total, including 16 (7%) of 214 hospitalised patients with COVID-19 in Wuhan, China, and 40 (69%) of 58 patients in intensive care with COVID-19 in France. Encephalitis has been described in eight patients to date, and Guillain-Barré syndrome in 19 patients. SARS-CoV-2 has been detected in the CSF of some patients. Anosmia and ageusia are common, and can occur in the absence of other clinical features. Unexpectedly, acute cerebrovascular disease is also emerging as an important complication, with cohort studies reporting stroke in 2-6% of patients hospitalised with COVID-19. So far, 96 patients with stroke have been described, who frequently had vascular events in the context of a pro-inflammatory hypercoagulable state with elevated C-reactive protein, D-dimer, and ferritin. WHERE NEXT?: Careful clinical, diagnostic, and epidemiological studies are needed to help define the manifestations and burden of neurological disease caused by SARS-CoV-2. Precise case definitions must be used to distinguish non-specific complications of severe disease (eg, hypoxic encephalopathy and critical care neuropathy) from those caused directly or indirectly by the virus, including infectious, para-infectious, and post-infectious encephalitis, hypercoagulable states leading to stroke, and acute neuropathies such as Guillain-Barré syndrome. Recognition of neurological disease associated with SARS-CoV-2 in patients whose respiratory infection is mild or asymptomatic might prove challenging, especially if the primary COVID-19 illness occurred weeks earlier. The proportion of infections leading to neurological disease will probably remain small. However, these patients might be left with severe neurological sequelae. With so many people infected, the overall number of neurological patients, and their associated health burden and social and economic costs might be large. Health-care planners and policy makers must prepare for this eventuality, while the many ongoing studies investigating neurological associations increase our knowledge base.
由严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)引起的 COVID-19 大流行是自 1918 年流感大流行以来未曾见过的规模。尽管主要的临床表现是呼吸道疾病,但神经系统表现越来越被认识到。根据对其他冠状病毒的了解,特别是那些引起严重急性呼吸系统综合征和中东呼吸系统综合征流行的冠状病毒,预计由 SARS-CoV-2 引起的中枢神经系统和周围神经系统疾病的病例会很少。
越来越多的病例报告和系列描述了 901 例患者的广泛神经系统表现,但许多报告的细节不够充分,反映了研究此类患者的挑战。共有 93 例患者报告了脑病,包括中国武汉 214 例 COVID-19 住院患者中的 16 例(7%)和法国重症监护 COVID-19 患者中的 40 例(69%)。迄今为止,已描述了 8 例脑炎和 19 例吉兰-巴雷综合征。一些患者的脑脊液中检测到了 SARS-CoV-2。嗅觉丧失和味觉丧失很常见,而且可能在没有其他临床特征的情况下发生。出乎意料的是,急性脑血管病也成为一个重要的并发症,队列研究报告 COVID-19 住院患者中有 2-6%发生中风。到目前为止,已经描述了 96 例中风患者,他们经常在炎症反应性高凝状态下出现血管事件,伴有 C 反应蛋白、D-二聚体和铁蛋白升高。
下一步是什么?需要进行仔细的临床、诊断和流行病学研究,以帮助确定由 SARS-CoV-2 引起的神经系统疾病的表现和负担。必须使用精确的病例定义来区分严重疾病的非特异性并发症(例如,缺氧性脑病和重症监护神经病)与直接或间接由病毒引起的并发症,包括感染性、副感染性和感染后脑炎、导致中风的高凝状态以及吉兰-巴雷综合征等急性神经病变。在呼吸道感染较轻或无症状的患者中识别与 SARS-CoV-2 相关的神经系统疾病可能具有挑战性,尤其是如果原发性 COVID-19 疾病发生在数周前。导致神经系统疾病的感染比例可能仍然很小。然而,这些患者可能会留下严重的神经系统后遗症。由于感染人数众多,患有神经系统疾病的患者以及他们相关的健康负担和社会经济成本可能会很大。卫生保健规划者和政策制定者必须为此做好准备,而许多正在进行的研究正在增加我们对神经系统关联的认识。