Malik Nabeela S, Chernbumroong Saisakul, Xu Yuanwei, Vassallo James, Lee Justine, Bowley Douglas M, Hodgetts Timothy, Moran Christopher G, Lord Janet M, Belli Antonio, Keene Damian, Foster Mark, Gkoutos Georgios V
NIHR Surgical Reconstruction and Microbiological Research Centre (SRMRC), Heritage Building, Queen Elizabeth Hospital, Mindelsohn Way, Edgbaston, Birmingham B15 2TH, UK.
Institute of Inflammation and Ageing, University of Birmingham, Birmingham B15 2TT, UK.
EClinicalMedicine. 2021 May 15;36:100888. doi: 10.1016/j.eclinm.2021.100888. eCollection 2021 Jun.
Natural disasters, conflict, and terrorism are major global causes of death and disability. Central to the healthcare response is triage, vital to ensure the right care is provided to the right patient at the right time. The ideal triage tool has high sensitivity for the highest priority (P1) patients with acceptably low over-triage. This study compared the performance of major incident triage tools in predicting P1 casualty status in adults in the prospective UK Trauma Audit and Research Network (TARN) registry.
TARN patients aged 16+ years (January 2008-December 2017) were included. Ten existing triage tools were applied using patients' first recorded pre-hospital physiology. Patients were subsequently assigned triage categories (P1, P2, P3, Expectant or Dead) based on pre-defined, intervention-based criteria. Tool performance was assessed by comparing tool-predicted and intervention-based priority status.
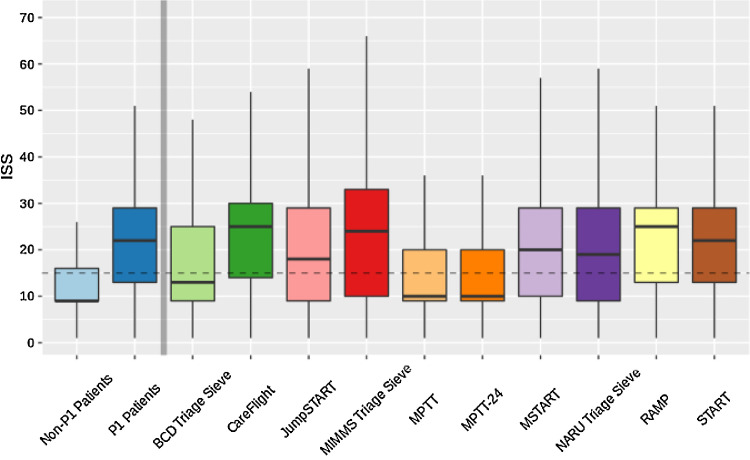
195,709 patients were included; mortality was 7·0% (n=13,601); median Injury Severity Score (ISS) was 9 (IQR 9-17); 97·1% sustained blunt injuries. 22,144 (11·3%) patients fulfilled intervention-based criteria for P1 status, exhibiting higher mortality (12·8% 5·0%, p<0.001), increased intensive care requirement (52·4% 5·0%, p<0.001), and more severe injuries (median ISS 21 9, p<0.001) compared with P2 patients.In 16-64 year olds, the highest performing tool was the Battlefield Casualty Drills (BCD) Triage Sieve (Prediction of P1 status: 70·4% sensitivity, over-triage 70·9%, area under the receiver operating curve (AUC) 0·068 [95%CI 0·676-0·684]). The UK National Ambulance Resilience Unit (NARU) Triage Sieve had sensitivity of 44·9%; over-triage 56·4%; AUC 0·666 (95%CI 0·662-0·670). All tools performed poorly amongst the elderly (65+ years).
The BCD Triage Sieve performed best in this nationally representative population; we recommend it supersede the NARU Triage Sieve as the UK primary major incident triage tool. Validated triage category definitions are recommended for appraising future major incidents.
This study is funded by the National Institute for Health Research (NIHR) Surgical Reconstruction and Microbiology Research Centre. GVG also acknowledges support from the MRC Heath Data Research UK (HDRUK/CFC/01). The views expressed are those of the authors and not necessarily those of the NIHR, the Department of Health and Social Care, or the Ministry of Defence.
自然灾害、冲突和恐怖主义是全球死亡和残疾的主要原因。医疗应对的核心是分诊,这对于确保在正确的时间为正确的患者提供正确的治疗至关重要。理想的分诊工具对最高优先级(P1)患者具有高灵敏度,同时过度分诊率可接受地低。本研究比较了主要事件分诊工具在英国前瞻性创伤审计与研究网络(TARN)登记处预测成人P1伤亡状况的性能。
纳入年龄在16岁及以上(2008年1月至2017年 December)的TARN患者。使用患者首次记录的院前生理数据应用十种现有的分诊工具。随后根据预定义的基于干预的标准为患者分配分诊类别(P1、P2、P3、预期或死亡)。通过比较工具预测的和基于干预的优先级状态来评估工具性能。
纳入195,709例患者;死亡率为7.0%(n = 13,601);中位损伤严重度评分(ISS)为9(四分位间距9 - 17);97.1%为钝性损伤。22,144例(11.3%)患者符合基于干预的P1状态标准,与P2患者相比,其死亡率更高(12.8%对5.0%,p < 0.001),重症监护需求增加(52.4%对5.0%,p < 0.001),损伤更严重(中位ISS 21对9,p < 0.001)。在16 - 64岁人群中,表现最佳的工具是战场伤亡演练(BCD)分诊筛检表(预测P1状态:灵敏度70.4%,过度分诊70.9%,受试者工作特征曲线下面积(AUC)0.68 [95%置信区间0.676 - 0.684])。英国国家救护车应急小组(NARU)分诊筛检表的灵敏度为44.9%;过度分诊56.4%;AUC 0.666(95%置信区间0.662 - 0.670)。所有工具在老年人(65岁及以上)中表现不佳。
BCD分诊筛检表在这个具有全国代表性的人群中表现最佳;我们建议它取代NARU分诊筛检表,成为英国主要事件的主要分诊工具。建议使用经过验证的分诊类别定义来评估未来的主要事件。
本研究由英国国家卫生研究院(NIHR)外科重建与微生物学研究中心资助。GVG还感谢医学研究委员会英国健康数据研究(HDRUK/CFC/01)的支持。所表达的观点是作者的观点,不一定代表NIHR、卫生与社会保健部或国防部的观点。