Institute of Hematology, Davidoff Center, Rabin Medical Center, Beilinson Hospital, Petach Tikva, Israel; Sackler School of Medicine, Aviv University, Aviv, Israel.
Institute of Hematology, Davidoff Center, Rabin Medical Center, Beilinson Hospital, Petach Tikva, Israel; Sackler School of Medicine, Aviv University, Aviv, Israel; Medicine A, Rabin Medical Center, Beilinson Hospital, Petach Tikva, Israel.
Haematologica. 2022 Mar 1;107(3):715-720. doi: 10.3324/haematol.2021.279216.
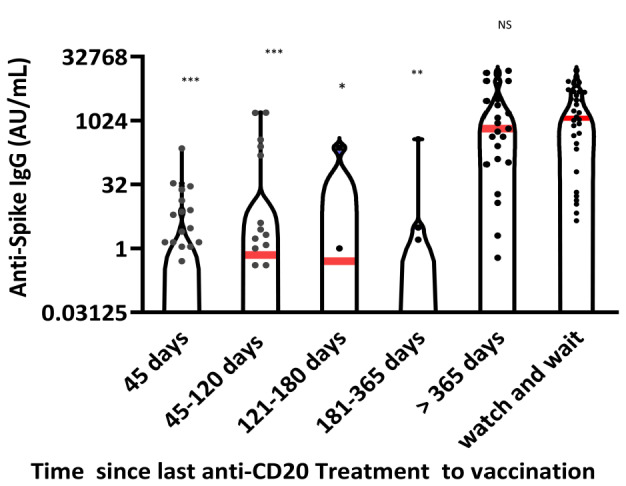
Patients with lymphoma, especially those treated with anti-CD20 monoclonal antibodies, suffer high COVID-19-associated morbidity and mortality. The goal of this study was to assess the ability of lymphoma patients to generate a sufficient humoral response after two injections of BNT162b2 Pfizer vaccine and to identify factors influencing the response. Antibody titers were measured with the SARS-CoV-2 IgG II Quant (Abbott ) assay in blood samples drawn from lymphoma patients 4 2 weeks after the second dose of vaccine. The cutoff for a positive response was set at 50 AU/mL. Positive serological responses were observed in 51% of the 162 patients enrolled in this cross-sectional study. In a multivariate analysis, an interval of <12 months between the last anti-CD20 monoclonal antibody dose and the second vaccine dose (odds ratio=31.3 [95% confidence interval: 8.4-116.9], P<0.001) and presence of active lymphoma (odds ratio=4.2 (95% confidence interval: 2.1- 8.2), P=0.006) were identified as negative response predictors. The rate of seropositivity increased from 3% in patients vaccinated within 45 days after the last monoclonal antibody administration to 80% in patients vaccinated >1 year after this therapy. The latter percentage was equal to that of patients never exposed to monoclonal antibodies. In conclusion, lymphoma patients, especially those recently treated with anti- CD20 monoclonal antibodies, fail to develop sufficient humoral response to BNT162b2 vaccine. While a serological response is not the only predictor of immunity, its low level could make this population more vulnerable to COVID-19, which implies the need for a different vaccination schedule for such patients.
淋巴瘤患者,尤其是接受抗 CD20 单克隆抗体治疗的患者,COVID-19 相关发病率和死亡率较高。本研究旨在评估淋巴瘤患者在接受两剂 BNT162b2 Pfizer 疫苗接种后产生足够体液反应的能力,并确定影响反应的因素。在第二次疫苗接种后 4 至 2 周,从淋巴瘤患者的血液样本中使用 SARS-CoV-2 IgG II Quant(雅培)测定法测量抗体滴度。将阳性反应的截止值设定为 50 AU/mL。在这项横断面研究中,纳入的 162 名患者中,有 51%观察到阳性血清学反应。在多变量分析中,最后一次抗 CD20 单克隆抗体剂量与第二次疫苗剂量之间的间隔<12 个月(比值比=31.3[95%置信区间:8.4-116.9],P<0.001)和存在活动性淋巴瘤(比值比=4.2[95%置信区间:2.1-8.2],P=0.006)被确定为阴性反应预测因素。血清阳性率从最后一次单克隆抗体给药后 45 天内接种疫苗的患者的 3%增加到接受治疗>1 年后接种疫苗的患者的 80%。后者的百分比与从未接受过单克隆抗体治疗的患者相同。总之,淋巴瘤患者,尤其是最近接受抗 CD20 单克隆抗体治疗的患者,无法对 BNT162b2 疫苗产生足够的体液反应。虽然血清学反应不是免疫的唯一预测因素,但低水平可能使该人群更容易感染 COVID-19,这意味着需要为此类患者制定不同的疫苗接种计划。