Clinical Epidemiology Division, Karolinska Institutet, Stockholm, Sweden.
Rheumatology, Karolinska University Hospital Solna, Stockholm, Sweden.
Rheumatology (Oxford). 2022 May 5;61(5):1810-1818. doi: 10.1093/rheumatology/keab570.
To estimate the occurrence and relative risks of first-ever-incident non-cutaneous cancer overall and for 16 sites in patients with RA treated with biologic and targeted synthetic DMARDs (b/tsDMARDs), by time since treatment start, attained age, and duration of active treatment.
This is an observational nationwide and population-based cohort study of patients with RA (n = 69 308), treated with TNF inhibitors (TNFi; adalimumab, certolizumab, etanercept, golimumab, infliximab) or other b/tsDMARDs (abatacept, rituximab, baricitinib, tofacitinib and tocilizumab) compared with RA patients not treated with b/tsDMARDs, and matched general population referents (n = 109 532), 2001-2018. The study was based on prospectively collected data from the Swedish Rheumatology Quality Register and from other registers, linked to the national Swedish Cancer Register. Incidence rates and hazard ratios were estimated via Cox regression adjusted for co-morbidities and other health characteristics.
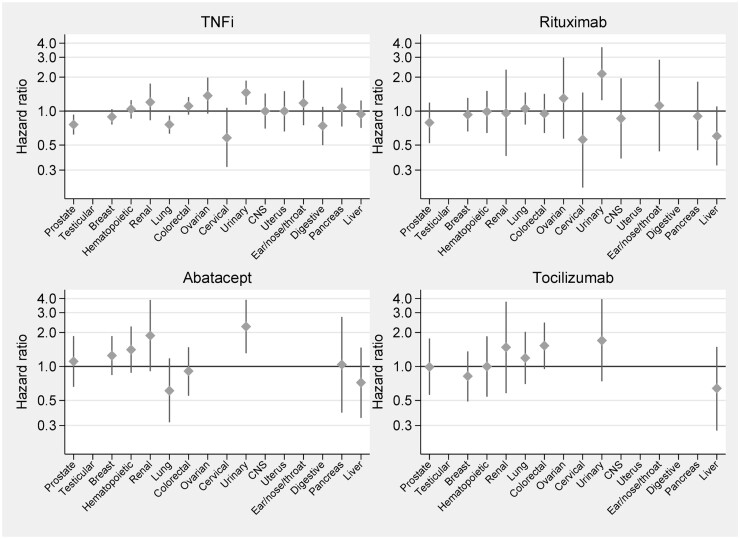
Based on 8633 incident cancers among RA patients, the overall relative risk of cancer with TNFi [hazard ratio (HR) = 1.0] was neither increased nor did it change with time since treatment start, duration of active treatment, or attained age, when compared with b/tsDMARD-naïve RA. For other b/tsDMARDs, we noted no consistent signal of increased overall risks (HRs ranged from 1.0 to 1.2), but there were statistically significant estimates above 1 for abatacept with 2-5 years of active treatment, for older age groups, and between several of the bDMARDs and urinary tract cancer.
TNFis, as used long term in clinical practice against RA, are not linked to increased risks for cancer overall. For other b/tsDMARDs, and for site-specific risks, our results are generally reassuring but contain signals that call for replication.
通过治疗起始时间、达到年龄和治疗活跃时间,评估接受生物制剂和靶向合成疾病修正抗风湿药物(b/tsDMARDs)治疗的类风湿关节炎(RA)患者中总体及 16 个部位首次发生非皮肤癌的发生率和相对风险。
这是一项观察性全国性和基于人群的 RA 患者队列研究(n=69308),他们接受了 TNF 抑制剂(TNFi;阿达木单抗、依那西普、依那西普、戈利木单抗、英夫利昔单抗)或其他 b/tsDMARDs(阿巴西普、利妥昔单抗、巴瑞替尼、托法替布和托珠单抗)治疗,与未接受 b/tsDMARDs 治疗的 RA 患者和匹配的一般人群参照者(n=109532)进行比较,时间范围为 2001-2018 年。该研究基于前瞻性收集的瑞典风湿病质量登记处和其他登记处的数据,并与全国瑞典癌症登记处相关联。通过 Cox 回归估计发病率和危险比,该回归模型调整了合并症和其他健康特征。
在 69308 例 RA 患者中,根据 8633 例癌症发病情况,与 b/tsDMARD 初治 RA 患者相比,TNFi 治疗后的总体癌症风险(危险比 [HR]=1.0)既未增加,也未随治疗起始时间、治疗活跃时间或达到年龄的变化而变化。对于其他 b/tsDMARDs,我们没有发现整体风险增加的一致信号(HR 范围为 1.0 至 1.2),但对于接受 2-5 年治疗的阿巴西普,以及年龄较大的人群和几种 bDMARDs 与尿路癌,估计值明显高于 1。
长期临床实践中使用的 TNFis 与总体癌症风险增加无关。对于其他 b/tsDMARDs 和特定部位的风险,我们的结果通常令人安心,但也包含需要进一步研究的信号。