Department of Hematology, Hyogo Prefectural Nishinomiya Hospital, 13-9, Rokutanji-cho, Nishinomiya, Hyogo, 662-0918, Japan.
Department of Rheumatology, Hyogo Prefectural Nishinomiya Hospital, Nishinomiya, Hyogo, Japan.
Int J Hematol. 2021 Nov;114(5):630-635. doi: 10.1007/s12185-021-03199-3. Epub 2021 Jul 30.
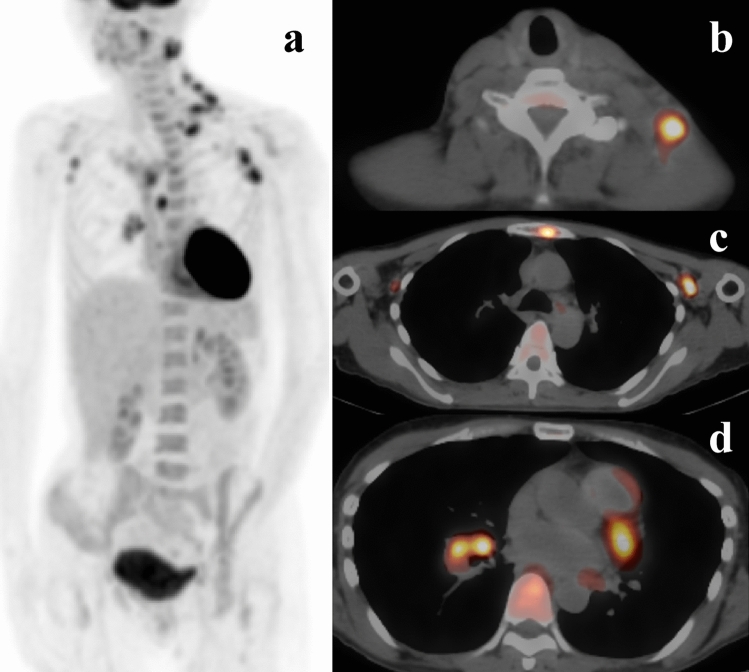
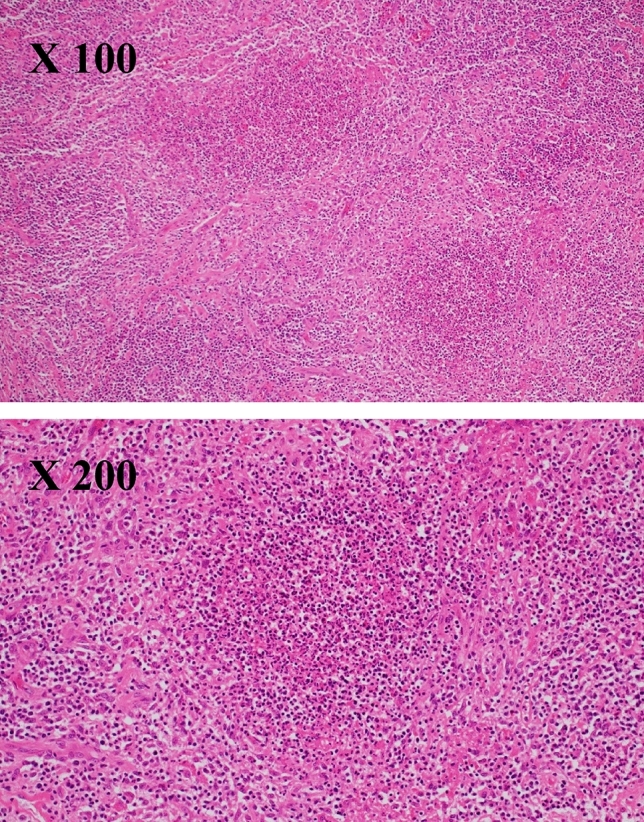
A previously healthy 49-year-old Japanese woman presented with cervical lymph node swelling and tenderness. Lymph node biopsy revealed reactive lymphadenitis without granulomas. No malignant cells were found, and no acid-fast positive bacilli were identified by Ziehl-Neelsen staining. She was treated unsuccessfully with various antibiotics, and it was very challenging to reach a diagnosis. F-Fluorodeoxyglucose (F-FDG) uptake in bones was evaluated using positron emission tomography-computed tomography (PET-CT), and disseminated mycobacterial infection was suspected. The interferon-gamma (IFN-γ) release assays QuantiFERON (QFT) and T-SPOT were used to diagnose tuberculosis infection. On testing, a difference in mitogen response was found between these assays. The response was low for QFT but adequate for T-SPOT, suggesting the presence of anti-IFN-γ antibodies. This difference depended on whether the patient's plasma (including anti-IFN-γ antibodies) was used within the assay system. Mycobacterium abscessus was isolated from lymph node cultures, and plasma anti-IFN-γ antibodies were confirmed. The patient was diagnosed with disseminated M. abscessus infection with underlying adult-onset immunodeficiency caused by anti-IFN-γ antibodies. Granulomas are a pathological hallmark of mycobacterial infection, but may not fully form in immunodeficient patients. Clinicians should be aware of the possibility of mycobacterial infection without granuloma formation due to anti-IFN-γ antibodies.
一位 49 岁的既往健康的日本女性出现颈部淋巴结肿大和触痛。淋巴结活检显示反应性淋巴结炎,无肉芽肿。Ziehl-Neelsen 染色未发现恶性细胞和抗酸阳性杆菌。她曾接受各种抗生素治疗,但均未成功,诊断极具挑战性。使用正电子发射断层扫描-计算机断层扫描(PET-CT)评估骨骼中 F-氟脱氧葡萄糖(F-FDG)摄取,怀疑为播散性分枝杆菌感染。干扰素-γ(IFN-γ)释放试验 QuantiFERON(QFT)和 T-SPOT 用于诊断结核感染。检测时,发现这些检测之间存在有丝分裂原反应的差异。QFT 的反应较低,但 T-SPOT 的反应足够,提示存在抗 IFN-γ 抗体。这种差异取决于是否在检测系统中使用了患者的血浆(包括抗 IFN-γ 抗体)。从淋巴结培养物中分离出脓肿分枝杆菌,并确认了血浆抗 IFN-γ 抗体。该患者被诊断为播散性 M.脓肿感染,其潜在的原因是由抗 IFN-γ 抗体引起的成人发病免疫缺陷。肉芽肿是分枝杆菌感染的病理标志,但在免疫功能低下的患者中可能不完全形成。临床医生应意识到由于抗 IFN-γ 抗体而导致无肉芽肿形成的分枝杆菌感染的可能性。