Center for Pharmacoepidemiology Research and Training, Center for Clinical Epidemiology and Biostatistics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Department of Biostatistics, Epidemiology and Informatics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Clin Pharmacol Ther. 2022 Jan;111(1):227-242. doi: 10.1002/cpt.2381. Epub 2021 Aug 17.
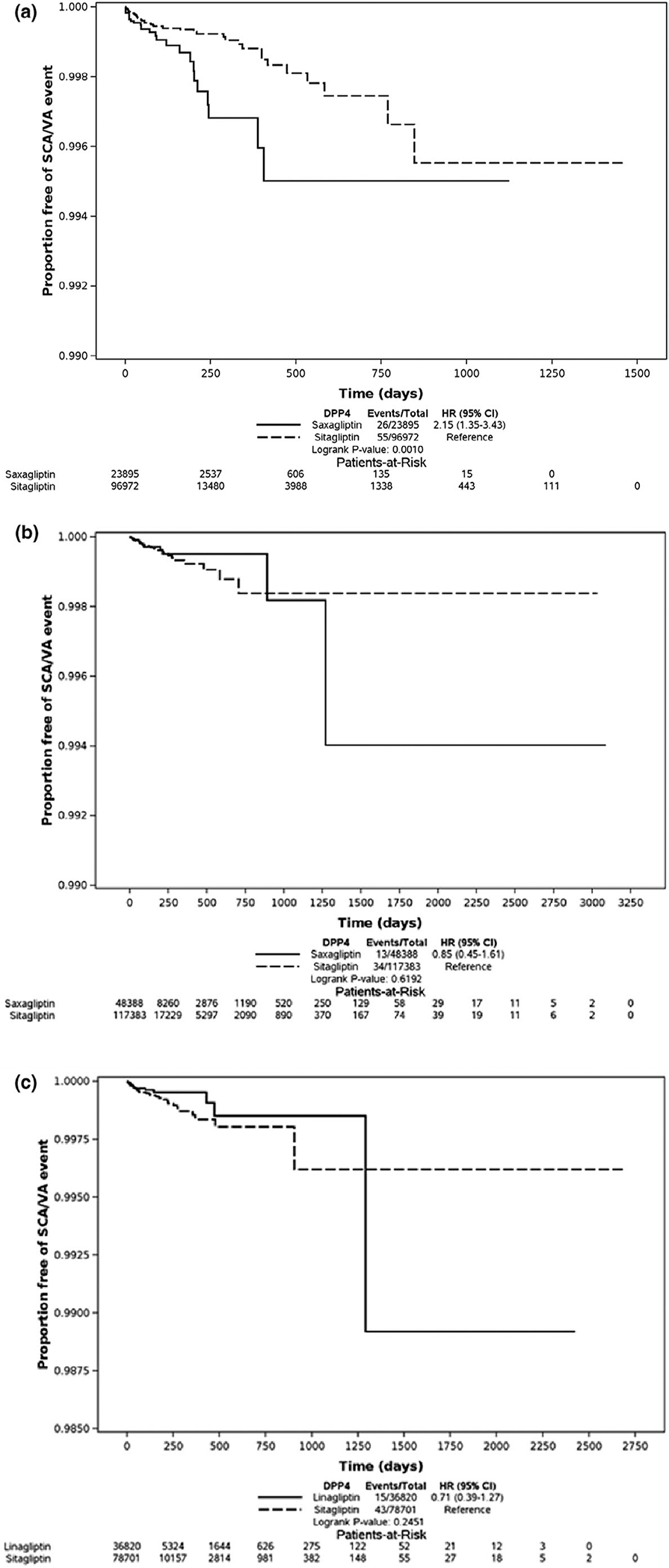
In vivo studies suggest that arrhythmia risk may be greater with less selective dipeptidyl peptidase-4 inhibitors, but evidence from population-based studies is missing. We aimed to compare saxagliptin, sitagliptin, and linagliptin with regard to risk of sudden cardiac arrest (SCA)/ventricular arrhythmia (VA). We conducted high-dimensional propensity score (hdPS) matched, new-user cohort studies. We analyzed Medicaid and Optum Clinformatics separately. We identified new users of saxagliptin, sitagliptin (both databases), and linagliptin (Optum only). We defined SCA/VA outcomes using emergency department and inpatient diagnoses. We identified and then controlled for confounders via a data-adaptive, hdPS approach. We generated marginal hazard ratios (HRs) via Cox proportional hazards regression using a robust variance estimator while adjusting for calendar year. We identified the following matched comparisons: saxagliptin vs. sitagliptin (23,895 vs. 96,972) in Medicaid, saxagliptin vs. sitagliptin (48,388 vs. 117,383) in Optum, and linagliptin vs. sitagliptin (36,820 vs. 78,701) in Optum. In Medicaid, use of saxagliptin (vs. sitagliptin) was associated with an increased rate of SCA/VA (adjusted HR (aHR), 2.01, 95% confidence interval (CI) 1.24-3.25). However, in Optum data, this finding was not present (aHR, 0.79, 95% CI 0.41-1.51). Further, we found no association between linagliptin (vs. sitagliptin) and SCA/VA (aHR, 0.65, 95% CI 0.36-1.17). We found discordant results regarding the association between SCA/VA with saxagliptin compared with sitagliptin in two independent datasets. It remains unclear whether these findings are due to heterogeneity of treatment effect in the different populations, chance, or unmeasured confounding.
体内研究表明,与选择性较低的二肽基肽酶-4 抑制剂相比,心律失常风险可能更高,但缺乏基于人群的研究证据。我们旨在比较沙格列汀、西他列汀和利拉利汀在心脏性猝死(SCA)/室性心律失常(VA)风险方面的差异。我们进行了高维倾向评分(hdPS)匹配的新用户队列研究。我们分别对医疗补助计划和 Optum Clinformatics 进行了分析。我们确定了沙格列汀、西他列汀(两个数据库)和利拉利汀(仅 Optum)的新使用者。我们使用急诊室和住院诊断来定义 SCA/VA 结局。我们通过数据自适应的 hdPS 方法识别并控制混杂因素。我们通过 Cox 比例风险回归生成边缘风险比(HR),使用稳健方差估计量,并根据日历年度进行调整。我们确定了以下匹配比较:医疗补助计划中沙格列汀与西他列汀(23895 对 96972),Optum 中沙格列汀与西他列汀(48388 对 117383),以及 Optum 中利拉利汀与西他列汀(36820 对 78701)。在医疗补助计划中,与西他列汀相比,使用沙格列汀与 SCA/VA 发生率增加相关(校正 HR(aHR),2.01,95%置信区间(CI)1.24-3.25)。然而,在 Optum 数据中,这一发现并不存在(aHR,0.79,95%CI 0.41-1.51)。此外,我们没有发现利拉利汀(与西他列汀相比)与 SCA/VA 之间存在关联(aHR,0.65,95%CI 0.36-1.17)。我们在两个独立的数据集之间发现了与沙格列汀相比,西他列汀与 SCA/VA 之间关联的不一致结果。这些发现是由于不同人群中治疗效果的异质性、偶然性还是未测量的混杂因素尚不清楚。