Vita-Salute San Raffaele University, Milan, Italy; Institute of Endocrine and Metabolic Sciences, IRCCS San Raffaele Hospital, Milan, Italy.
Vita-Salute San Raffaele University, Milan, Italy; Division of Immunology, Transplantation and Infectious Diseases, IRCCS San Raffaele Scientific Institute, Milan, Italy.
Diabetes Metab. 2021 Nov;47(6):101268. doi: 10.1016/j.diabet.2021.101268. Epub 2021 Jul 29.
Obesity is a risk factor for COVID-19, but the underlying mechanisms are unclear. We investigated the role of adiponectin (an anti-inflammatory adipokine), leptin (a pro-inflammatory adipokine) and their ratio (Adpn/Lep) in this context.
Single-centre, prospective observational study.
Adiponectin and leptin were measured in 60 COVID-19 patients with mild (not hospitalised, n=11), moderate (hospitalised but not requiring intensive care, n=25) and severe (admission to the intensive care unit [ICU] or death, n=24) disease.
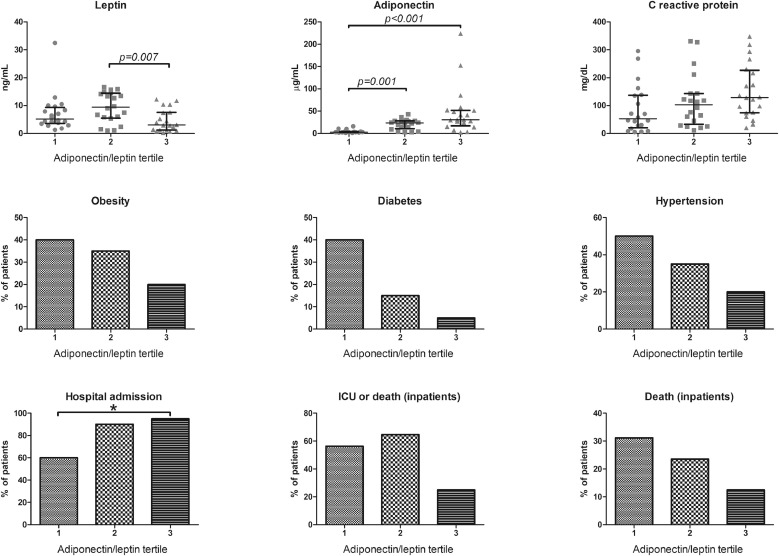
Adiponectin and leptin levels were similar across severity groups, but patients with moderate severity had the highest Adpn/Lep ratio (1.2 [0.5; 2.0], 5.0 [1.6; 11.2], 2.1 [1.0; 3.6] in mild, moderate and severe disease; P = 0.019). Adpn/Lep, but not adiponectin or leptin alone, correlated with systemic inflammation (C reactive protein, CRP: Spearman's rho 0.293, P = 0.023). When dividing patients into Adpn/Lep tertiles, adiponectin was highest, whereas leptin was lowest in the third (highest) tertile. Patients in the highest Adpn/Lep tertile had numerically lower rates of obesity, diabetes and hypertension, and lower rates of death or admission to ICU versus other tertiles. At linear regression in the whole cohort, CRP significantly predicted Adpn/Lep (β 0.291, P = 0.022), while female gender (β -0.289, P = 0.016), diabetes (β -0.257, P = 0.028), and hypertension (β -239, P = 0.043) were negative predictors.
We speculate that the rise in Adpn/Lep, due to increased adiponectin and reduced leptin, is a compensatory response to systemic inflammation. In patients with worse cardiometabolic health (e.g. diabetes, hypertension) this mechanism might be blunted, possibly contributing to higher mortality.
肥胖是 COVID-19 的一个风险因素,但潜在机制尚不清楚。我们研究了脂联素(一种抗炎脂肪因子)、瘦素(一种促炎脂肪因子)及其比值(Adpn/Lep)在这种情况下的作用。
单中心、前瞻性观察性研究。
测量了 60 名 COVID-19 患者的脂联素和瘦素水平,这些患者的疾病严重程度为轻度(未住院,n=11)、中度(住院但不需要重症监护,n=25)和重度(入住重症监护病房[ICU]或死亡,n=24)。
脂联素和瘦素水平在严重程度组之间相似,但中度严重程度的患者具有最高的 Adpn/Lep 比值(1.2[0.5;2.0]、5.0[1.6;11.2]、2.1[1.0;3.6],轻度、中度和重度疾病;P=0.019)。Adpn/Lep 与全身炎症相关(C 反应蛋白,CRP:Spearman's rho 0.293,P=0.023),但脂联素或瘦素单独不相关。当将患者按 Adpn/Lep 三分位数分组时,第三(最高)三分位数的脂联素最高,而瘦素最低。Adpn/Lep 最高三分位数的患者肥胖、糖尿病和高血压的发生率较低,与其他三分位数相比,死亡率或 ICU 入院率也较低。在整个队列的线性回归中,CRP 显著预测 Adpn/Lep(β 0.291,P=0.022),而女性(β -0.289,P=0.016)、糖尿病(β -0.257,P=0.028)和高血压(β -239,P=0.043)是负预测因子。
我们推测,由于脂联素增加和瘦素减少,Adpn/Lep 的升高是对全身炎症的代偿反应。在合并较差的心血管代谢健康(如糖尿病、高血压)的患者中,这种机制可能受到抑制,可能导致更高的死亡率。