Shiwaku Eiji, Dote Satoshi, Kaneko Shinobu, Hei Chisato, Aikawa Masaki, Sakai Yuki, Kawai Takahiro, Iwatsubo Shigeaki, Hashimoto Michinobu, Tsuneishi Teppei, Nishimura Tomoko, Iwata Toshiyuki, Hira Daiki, Terada Tomohiro, Nishimura Takashi, Kobayashi Yuka
Department of Pharmacy, Kyoto-Katsura Hospital, 17, Yamadahiraocho, Kyoto-shi Nishikyo-ku, Kyoto, 615-8256, Japan.
Department of Respiratory Medicine, Kyoto-Katsura Hospital, Kyoto, Japan.
J Pharm Health Care Sci. 2021 Aug 2;7(1):28. doi: 10.1186/s40780-021-00211-0.
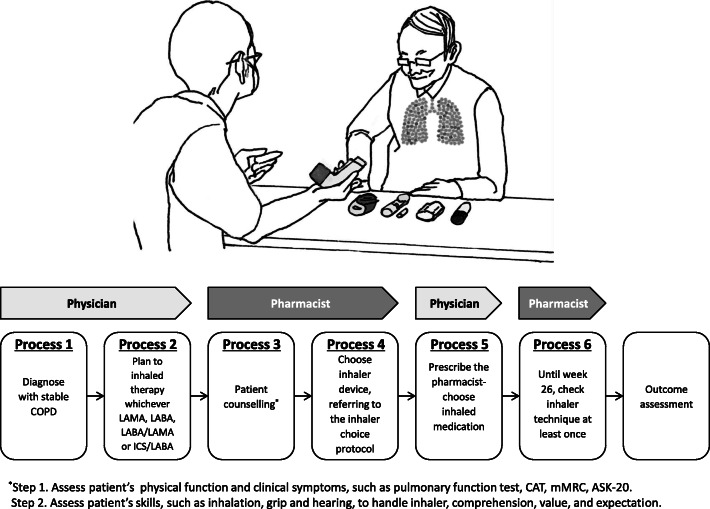
Currently, in Japan, shifting tasks from physician to hospital pharmacist is being developed to reduce physician workload and improve the quality of pharmacotherapy. This study aimed to investigate the effects of pharmacist involvement in the choice of inhaler as the task on the clinical outcomes of patients with chronic obstructive pulmonary disease (COPD).
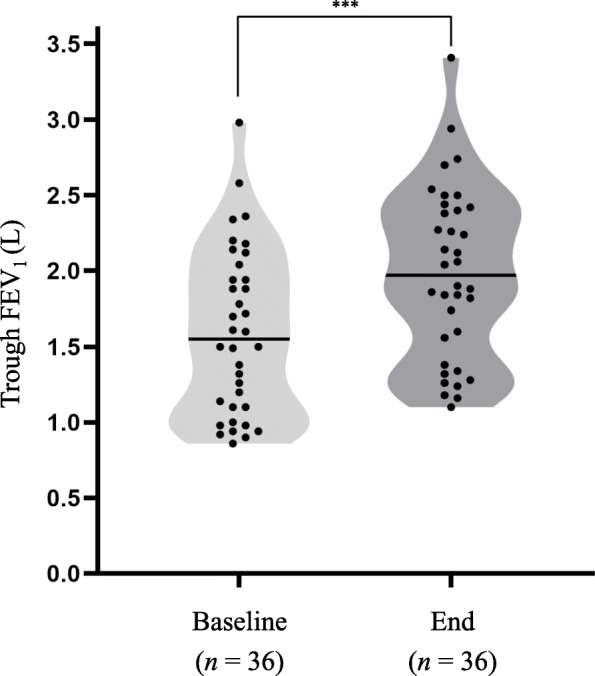
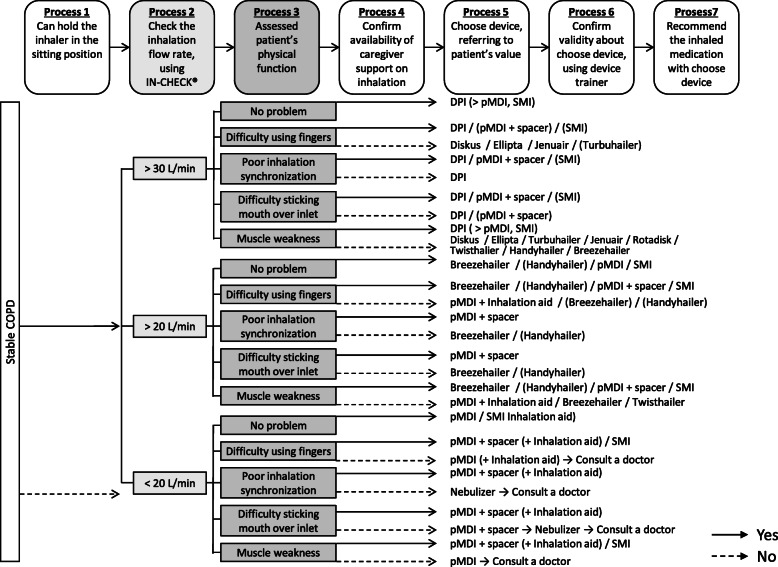
This prospective, single-center, single-arm study included 36 outpatients with newly diagnosed COPD indicating inhaler therapy. Eligible patients were immediately interviewed by pharmacist. Then, pharmacist assessed patient's inhalation flow rate, physical function to handle an inhaler, comprehension, and value, and finally recommended a personalized inhaler based on originally developed inhaler choice protocol, and pulmonologist prescribed a pharmacist-selected inhaler. The primary endpoint was the improvement in trough forced expiratory volume in 1 s (FEV) between baseline and week 26. The secondary endpoints were safety, and improvements at week 26 in scores for the COPD Assessment Test (CAT), modified British Medical Research Council Dyspnea Scale (mMRC), and Adherence Starts with Knowledge-20 (ASK-20).
The pneumonologists completely agreed with the pharmacist-recommended inhaler. Mean FEV significantly increased from baseline to week 26 (1.60, SD 0.54 L vs. 1.98, SD 0.56 L; p < 0.0001). Significant improvements in CAT, mMRC, and ASK-20 scores were also observed. The prevalence of CAT responders as a negative predictor of acute exacerbation, defined as those with a decrease in CAT score of ≥2 points from baseline, was 86%. None of the patients experienced exacerbation during the study period.
Pharmacist involvement in the choice of inhaler for patients with newly diagnosed COPD was associated with improved lung function, health status, clinical symptoms, and adherence to inhaler therapy. Shifting task of choosing appropriate inhaler from physician to hospital pharmacist may be performed effectively and safely with an inhaler choice protocol.
UMIN000039722 , retrospectively registered on March 10, 2020.
目前在日本,为减轻医生工作量并提高药物治疗质量,正致力于将任务从医生转移至医院药剂师。本研究旨在调查药剂师参与吸入器选择任务对慢性阻塞性肺疾病(COPD)患者临床结局的影响。
这项前瞻性、单中心、单臂研究纳入了36例新诊断为COPD且需吸入器治疗的门诊患者。符合条件的患者立即接受药剂师的访谈。然后,药剂师评估患者的吸入流速、操作吸入器的身体功能、理解能力和价值观,最后根据最初制定的吸入器选择方案推荐个性化吸入器,肺科医生开具药剂师选择的吸入器。主要终点是基线至第26周期间1秒用力呼气容积(FEV)的改善情况。次要终点是安全性,以及第26周时慢性阻塞性肺疾病评估测试(CAT)、改良英国医学研究委员会呼吸困难量表(mMRC)和知识促进依从性-20(ASK-20)评分的改善情况。
肺科医生完全同意药剂师推荐的吸入器。从基线到第26周,平均FEV显著增加(1.60,标准差0.54L对1.98,标准差0.56L;p<0.0001)。CAT、mMRC和ASK-20评分也有显著改善。作为急性加重的阴性预测指标,CAT应答者(定义为CAT评分较基线降低≥2分者)的患病率为86%。在研究期间,没有患者出现病情加重。
药剂师参与新诊断COPD患者吸入器的选择与肺功能、健康状况、临床症状改善以及吸入器治疗依从性提高有关。通过吸入器选择方案,将选择合适吸入器的任务从医生转移至医院药剂师可能是有效且安全的。
UMIN000039722,于2020年3月10日进行回顾性注册。