Centre de Pneumologie, Institut universitaire de cardiologie et de pneumologie de Québec, Université Laval, Québec, Canada.
Respiratory Medicine and Allergology, Lund University, Lund, Sweden.
Respir Res. 2019 Oct 30;20(1):238. doi: 10.1186/s12931-019-1193-9.
Prospective evidence is lacking regarding incremental benefits of long-acting dual- versus mono-bronchodilation in improving symptoms and preventing short-term disease worsening/treatment failure in low exacerbation risk patients with chronic obstructive pulmonary disease (COPD) not receiving inhaled corticosteroids.
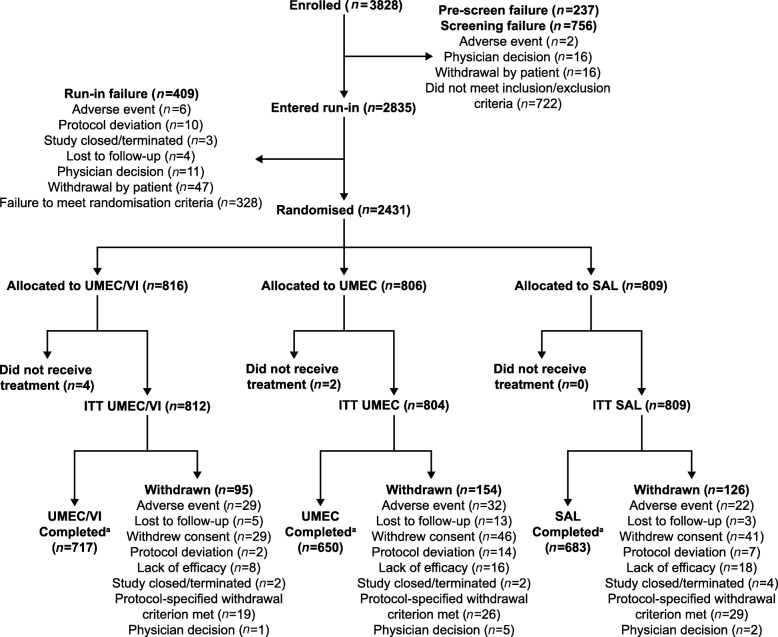
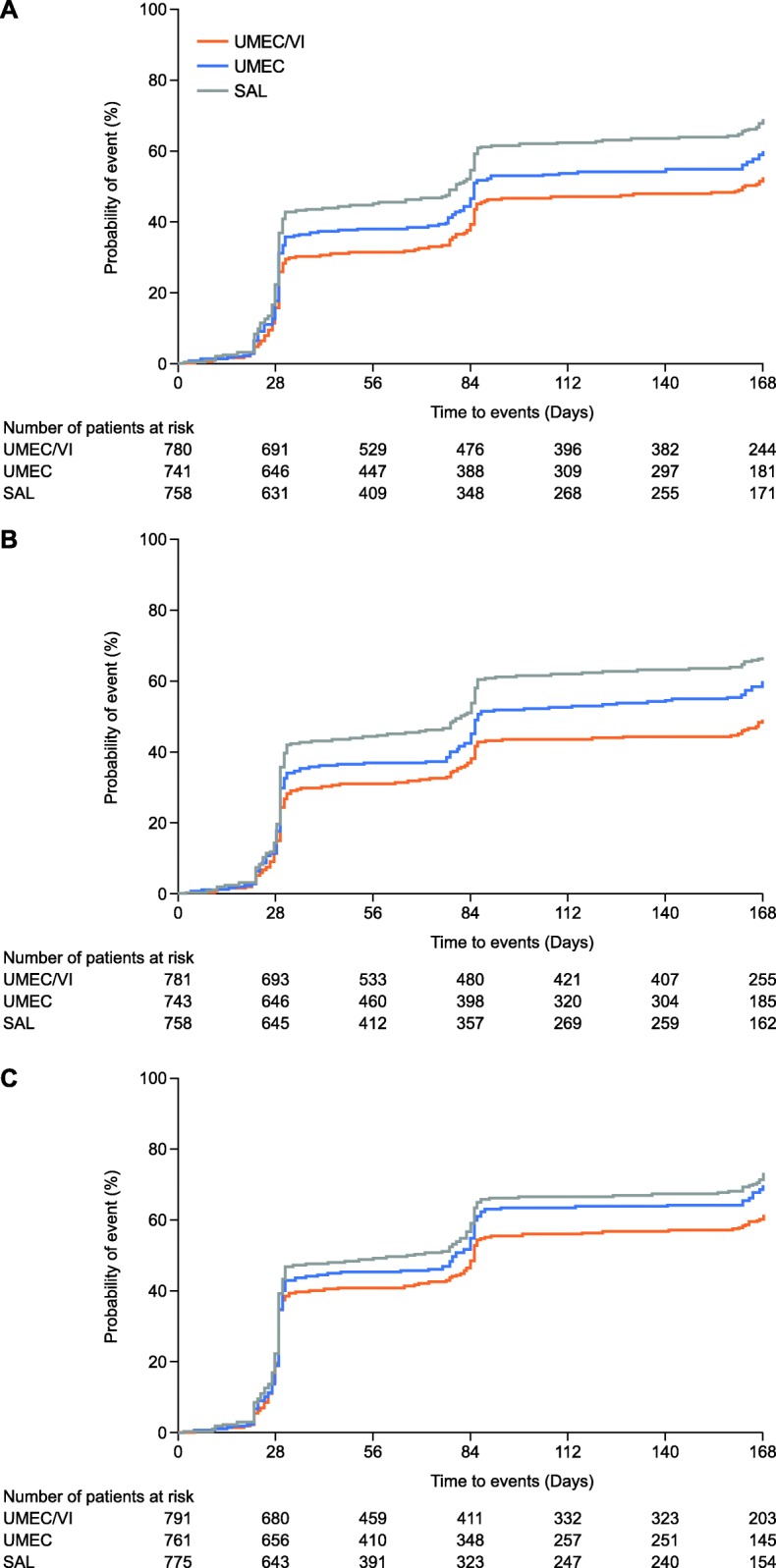
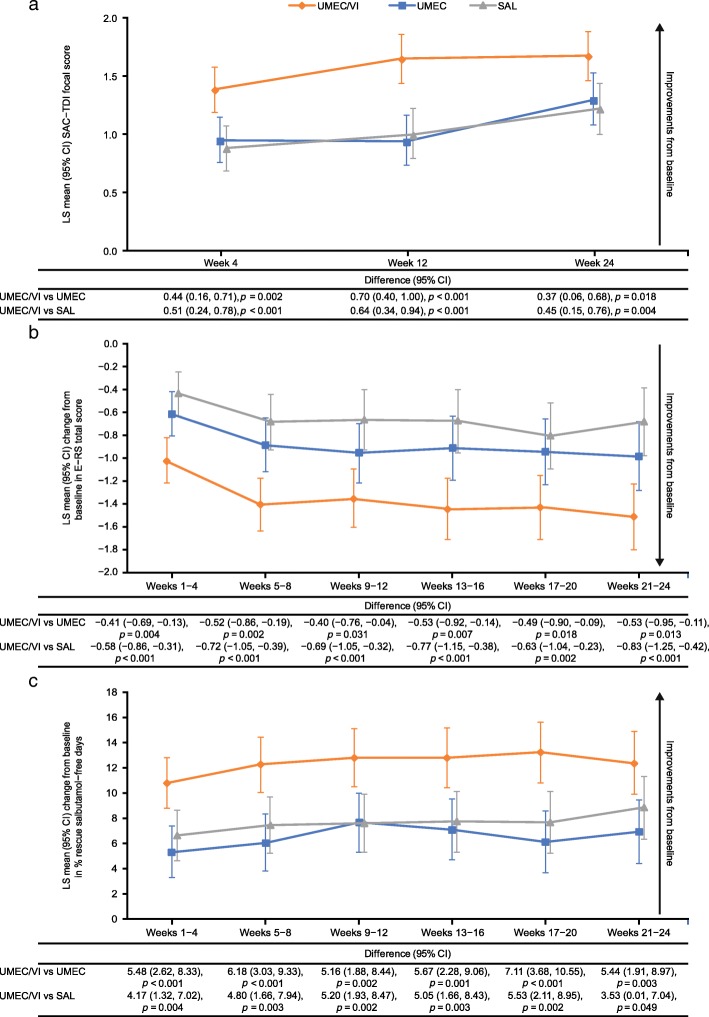
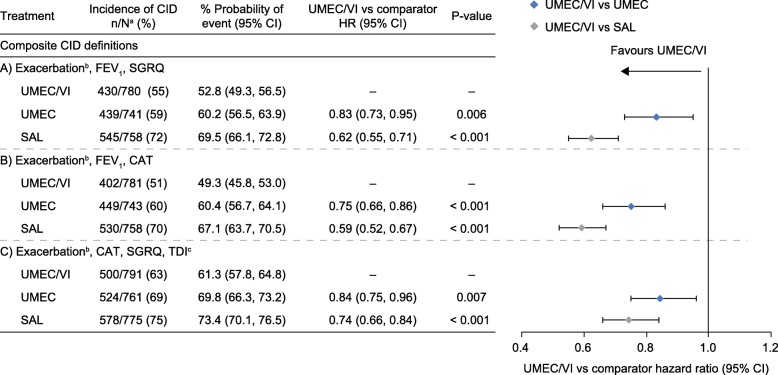
The 24-week, double-blind, double-dummy, parallel-group Early MAXimisation of bronchodilation for improving COPD stability (EMAX) trial randomised patients at low exacerbation risk not receiving inhaled corticosteroids, to umeclidinium/vilanterol 62.5/25 μg once-daily, umeclidinium 62.5 μg once-daily or salmeterol 50 μg twice-daily. The primary endpoint was trough forced expiratory volume in 1 s (FEV) at Week 24. The study was also powered for the secondary endpoint of Transition Dyspnoea Index at Week 24. Other efficacy assessments included spirometry, symptoms, heath status and short-term disease worsening measured by the composite endpoint of clinically important deterioration using three definitions.
Change from baseline in trough FEV at Week 24 was 66 mL (95% confidence interval [CI]: 43, 89) and 141 mL (95% CI: 118, 164) greater with umeclidinium/vilanterol versus umeclidinium and salmeterol, respectively (both p < 0.001). Umeclidinium/vilanterol demonstrated consistent improvements in Transition Dyspnoea Index versus both monotherapies at Week 24 (vs umeclidinium: 0.37 [95% CI: 0.06, 0.68], p = 0.018; vs salmeterol: 0.45 [95% CI: 0.15, 0.76], p = 0.004) and all other symptom measures at all time points. Regardless of the clinically important deterioration definition considered, umeclidinium/vilanterol significantly reduced the risk of a first clinically important deterioration compared with umeclidinium (by 16-25% [p < 0.01]) and salmeterol (by 26-41% [p < 0.001]). Safety profiles were similar between treatments.
Umeclidinium/vilanterol consistently provides early and sustained improvements in lung function and symptoms and reduces the risk of deterioration/treatment failure versus umeclidinium or salmeterol in symptomatic patients with low exacerbation risk not receiving inhaled corticosteroids. These findings suggest a potential for early use of dual bronchodilators to help optimise therapy in this patient group.
在没有吸入皮质激素的低加重风险慢性阻塞性肺疾病(COPD)患者中,长效双支气管扩张剂与单支气管扩张剂相比,在改善症状和预防短期疾病恶化/治疗失败方面的额外获益尚缺乏前瞻性证据。
24 周、双盲、双模拟、平行组早期最大程度改善 COPD 稳定的支气管扩张(EMAX)试验将低加重风险未接受吸入皮质激素的患者随机分配至乌美溴铵/维兰特罗 62.5/25μg 每日一次、乌美溴铵 62.5μg 每日一次或沙美特罗 50μg 每日两次。主要终点为第 24 周时的谷值用力呼气 1 秒量(FEV1)。该研究也有能力检测次要终点第 24 周时的过渡呼吸困难指数。其他疗效评估包括肺量计、症状、健康状况和使用三种定义的临床重要恶化的复合终点测量的短期疾病恶化。
与乌美溴铵相比,乌美溴铵/维兰特罗在第 24 周时的谷值 FEV1 分别增加了 66mL(95%置信区间[CI]:43,89)和 141mL(95%CI:118,164)(均 p<0.001)。与两种单药治疗相比,乌美溴铵/维兰特罗在第 24 周时在过渡呼吸困难指数上表现出一致的改善(与乌美溴铵相比:0.37[95%CI:0.06,0.68],p=0.018;与沙美特罗相比:0.45[95%CI:0.15,0.76],p=0.004),并且在所有时间点的所有其他症状测量上均有改善。无论考虑哪种临床重要恶化定义,与乌美溴铵相比,乌美溴铵/维兰特罗均显著降低了首次临床重要恶化的风险(降低 16%-25%[p<0.01]),与沙美特罗相比(降低 26%-41%[p<0.001])。治疗之间的安全性特征相似。
与乌美溴铵或沙美特罗相比,乌美溴铵/维兰特罗可持续改善低加重风险、未接受吸入皮质激素的 COPD 患者的肺功能和症状,并降低恶化/治疗失败的风险。这些发现表明,在该患者群体中,早期使用双支气管扩张剂可能有助于优化治疗。