Department of Emergency and Critical Care Medicine, Kanazawa University Hospital, Kanazawa.
Department of Cardiology, Osaka Saiseikai Senri Hospital, Suita.
Eur J Emerg Med. 2022 Feb 1;29(1):42-48. doi: 10.1097/MEJ.0000000000000861.
Bystander cardiopulmonary resuscitation (CPR) and initial shockable rhythm are crucial predictors of survival after out-of-hospital cardiac arrest (OHCA). However, the relationship between dispatcher-assisted CPR (DA-CPR) and initial shockable rhythm is not completely elucidated.
To examine the association of DA-CPR with initial shockable rhythm and outcomes.
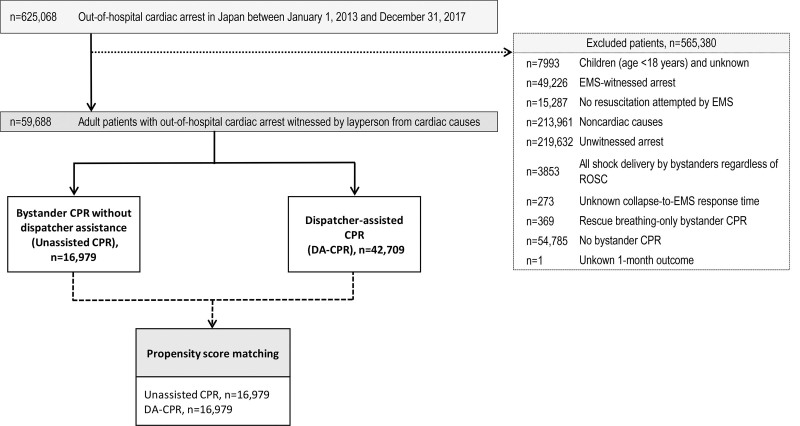
DESIGN, SETTING AND PARTICIPANTS: This nationwide population-based observational study conducted in Japan included 59 688 patients with witnessed OHCA of cardiac origin after excluding those without bystander CPR. Patients were divided into DA-CPR (n = 42 709) and CPR without dispatcher assistance (unassisted CPR, n = 16 979) groups.
The primary outcome measure was initial shockable rhythm, and secondary outcome measures were 1-month survival and neurologically intact survival. A Cox proportional hazards model adjusted for collapse-to-first-rhythm-analysis time and multivariable logistic regression models were used after propensity score (PS) matching to compare the incidence of initial shockable rhythm and outcomes, respectively.
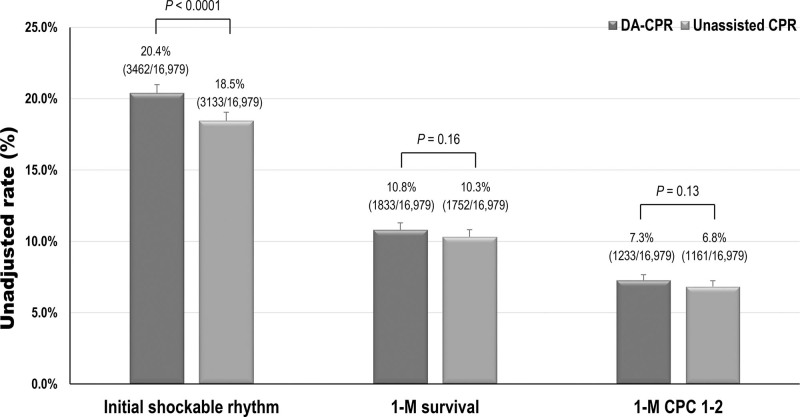
Among all patients (mean age 76.7 years), the rates of initial shockable rhythm, 1-month survival and neurologically intact survival were 20.8, 10.7 and 7.0%, respectively. The incidence of initial shockable rhythm in the DA-CPR group (20.4%, 3462/16 979) was significantly higher than that in the unassisted CPR group (18.5%, 3133/16 979) after PS matching (P < 0.0001). However, no significant differences were found between the two groups with respect to the incidence of initial shockable rhythm in the Cox proportional hazards model [adjusted hazard ratio of DA-CPR for initial shockable rhythm compared with unassisted CPR, 0.99; 95% confidence interval (CI), 0.97-1.02, P = 0.56]. No significant differences were observed in the survival rates in the two groups after PS matching [10.8% (1833/16 979) vs. 10.3% (1752/16 979), P = 0.16] and neurologically intact survival rates [7.3% (1233/16 979) vs. 6.8% (1161/16 979), P = 0.13]. The multivariable logistic regression model showed no significant differences between the groups with regard to survival (adjusted odds ratio of DA-CPR compared with unassisted CPR: 1.00; 95% CI, 0.89-1.13, P = 0.97) and neurologically intact survival (adjusted odds ratio: 1.12; 95% CI, 0.98-1.29, P = 0.14).
DA-CPR after OHCA had the same independent association with the likelihood of initial shockable rhythm and 1-month meaningful outcome as unassisted CPR.
院外心脏骤停(OHCA)后旁观者心肺复苏(CPR)和初始可除颤节律是生存的重要预测因素。然而,调度员协助的 CPR(DA-CPR)与初始可除颤节律之间的关系尚未完全阐明。
研究 DA-CPR 与初始可除颤节律和结局之间的关系。
设计、地点和参与者:本研究在日本进行了一项全国范围内的基于人群的观察性研究,纳入了 59688 例有目击者的心脏原因 OHCA 患者,排除了无旁观者 CPR 的患者。患者分为 DA-CPR(n=42709)和无调度员协助的 CPR(非协助性 CPR,n=16979)组。
主要结局测量指标为初始可除颤节律,次要结局测量指标为 1 个月生存率和神经功能完整生存率。使用 Cox 比例风险模型调整了从心脏骤停到首次节律分析的时间,并在倾向评分(PS)匹配后使用多变量逻辑回归模型分别比较了初始可除颤节律和结局的发生率。
在所有患者中(平均年龄 76.7 岁),初始可除颤节律、1 个月生存率和神经功能完整生存率的发生率分别为 20.8%、10.7%和 7.0%。在 PS 匹配后,DA-CPR 组(20.4%,3462/16979)的初始可除颤节律发生率明显高于非协助性 CPR 组(18.5%,3133/16979)(P<0.0001)。然而,在 Cox 比例风险模型中,两组之间初始可除颤节律的发生率没有显著差异[DA-CPR 与非协助性 CPR 相比初始可除颤节律的调整后危险比,0.99;95%置信区间(CI),0.97-1.02,P=0.56]。在 PS 匹配后,两组的生存率[10.8%(1833/16979)与 10.3%(1752/16979),P=0.16]和神经功能完整生存率[7.3%(1233/16979)与 6.8%(1161/16979),P=0.13]没有显著差异。多变量逻辑回归模型显示,两组在生存率[DA-CPR 与非协助性 CPR 的调整后比值比,1.00;95%CI,0.89-1.13,P=0.97]和神经功能完整生存率[调整后比值比,1.12;95%CI,0.98-1.29,P=0.14]方面没有显著差异。
OHCA 后 DA-CPR 与初始可除颤节律和 1 个月有意义结局的可能性具有相同的独立关联,与非协助性 CPR 相同。