Department of Emergency and Critical Care Medicine, Kanazawa University Hospital, Takaramachi 13-1, Kanazawa, 920-8640, Japan.
Department of Cardiology, Osaka Saiseikai Senri Hospital, Tukumodai 1-1-6, Suita, 565-0862, Japan.
Crit Care. 2021 Nov 27;25(1):408. doi: 10.1186/s13054-021-03825-w.
The International Liaison Committee on Resuscitation recommends that dispatchers provide instructions to perform compression-only cardiopulmonary resuscitation (CPR) to callers responding to adults with out-of-hospital cardiac arrest (OHCA). This study aimed to determine the optimal dispatcher-assisted CPR (DA-CPR) instructions for OHCA.
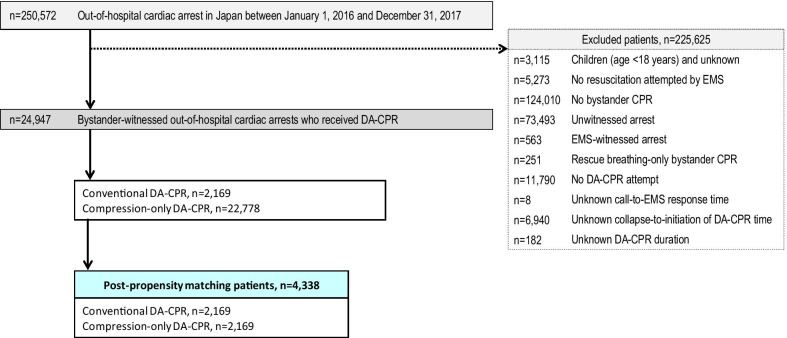
We analysed the records of 24,947 adult patients (aged ≥ 18 years) who received bystander DA-CPR after bystander-witnessed OHCA. Data were obtained from a prospectively recorded Japanese nationwide Utstein-style database for a 2-year period (2016-2017). Patients were divided into compression-only DA-CPR (n = 22,778) and conventional DA-CPR (with a compression-to-ventilation ratio of 30:2, n = 2169) groups. The primary outcome measure was 1-month neurological intact survival, defined as a cerebral performance category score of 1-2 (CPC 1-2).
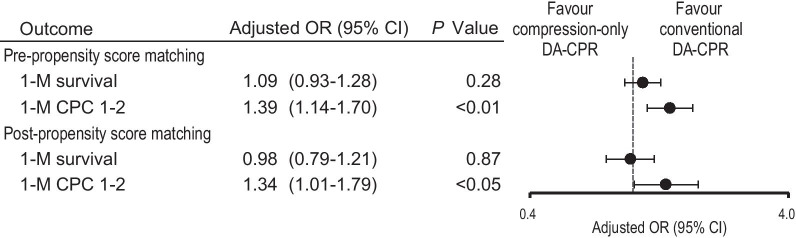
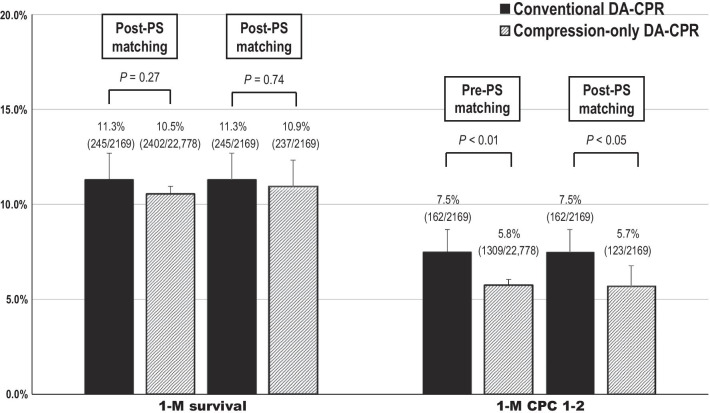
The 1-month CPC 1-2 rate was significantly higher in the conventional DA-CPR group than in the compression-only DA-CPR group (before propensity score (PS) matching, 7.5% [162/2169] versus 5.8% [1309/22778], p < 0.01; after PS matching, 7.5% (162/2169) versus 5.7% (123/2169), p < 0.05). Compared with compression-only DA-CPR, conventional DA-CPR was associated with increased odds of 1-month CPC 1-2 (before PS matching, adjusted odds ratio 1.39, 95% confidence interval [CI] 1.14-1.70, p < 0.01; after PS matching, adjusted odds ratio 1.34, 95% CI 1.00-1.79, p < 0.05).
Within the limitations of this retrospective observational study, conventional DA-CPR with a compression-to-ventilation ratio of 30:2 was preferable to compression-only DA-CPR as an optimal DA-CPR instruction for coaching callers to perform bystander CPR for adult patients with bystander-witnessed OHCAs.
国际复苏联合会建议调度员向响应院外心脏骤停(OHCA)的呼叫者提供仅进行按压的心肺复苏(CPR)指导。本研究旨在确定 OHCA 的最佳调度员辅助 CPR(DA-CPR)指导。
我们分析了 24947 名接受旁观者 DA-CPR 的成年患者(年龄≥18 岁)的记录,这些患者在旁观者目击 OHCA 后接受了旁观者 DA-CPR。数据来自一个前瞻性记录的日本全国性乌斯丁式数据库,为期 2 年(2016-2017 年)。患者分为仅按压 DA-CPR(n=22778)和常规 DA-CPR(按压通气比为 30:2,n=2169)组。主要结局指标是 1 个月时神经功能完整存活,定义为脑功能分类评分 1-2 级(CPC 1-2)。
在常规 DA-CPR 组中,1 个月时 CPC 1-2 率明显高于仅按压 DA-CPR 组(在进行倾向评分(PS)匹配之前,7.5%[162/2169]与 5.8%[1309/22778],p<0.01;在进行 PS 匹配后,7.5%[162/2169]与 5.7%[123/2169],p<0.05)。与仅按压 DA-CPR 相比,常规 DA-CPR 与 1 个月时 CPC 1-2 的可能性增加相关(在 PS 匹配之前,调整后的优势比 1.39,95%置信区间 [CI] 1.14-1.70,p<0.01;在 PS 匹配后,调整后的优势比 1.34,95% CI 1.00-1.79,p<0.05)。
在本回顾性观察研究的限制内,与仅按压 DA-CPR 相比,30:2 的常规 DA-CPR 作为指导呼叫者对旁观者目击的 OHCA 成年患者进行旁观者 CPR 的最佳 DA-CPR 指导更可取。