Allergy Unit, Department of Pediatrics, Meyer Children's University Hospital, Florence, Italy.
Dermatology Unit, Department of Pediatrics, Meyer Children's University Hospital, Florence, Italy.
Front Immunol. 2021 Jul 15;12:688364. doi: 10.3389/fimmu.2021.688364. eCollection 2021.
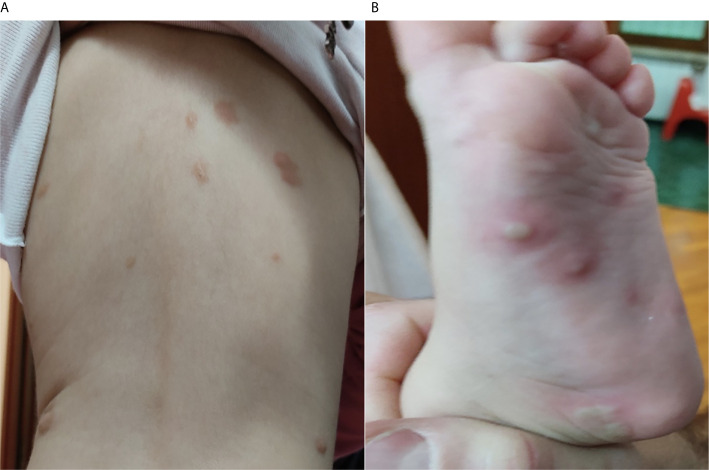
Vaccination is a well-known trigger for mast cell degranulation in subjects affected by mastocytosis. Nevertheless, there is no exact standardized protocol to prevent a possible reaction after a vaccine injection, especially for patients who have already presented a previous vaccine-related adverse event, considering that these patients frequently tolerate future vaccine doses. For this reason, we aim to share our experience at Meyer Children's University Hospital in Florence to raise awareness on the potential risk for future vaccinations and to discuss the valuable therapeutic strategies intended to prevent them, taking into account what is proposed by experts in literature. We describe the case of an 18-month-old female affected by a polymorphic variant of maculopapular cutaneous mastocytosis that presented an extensive bullous cutaneous reaction 24 hours after the second dose (booster dose) of inactivated-tetravalent influenza vaccine, treated with a single dose of oral corticosteroid therapy with betamethasone (0.1 mg/kg) and an oral antihistamine therapy with oxatomide (1 mg/kg/daily) for a week, until resolution. To the best of our knowledge, in the literature, no documented case of reaction to influenza vaccine in maculopapular cutaneous mastocytosis is described. Subsequently, the patient started a background therapy with ketotifen daily (0.05 mg/kg twice daily), a non-competitive H1-antihistamine, and a mast cell stabilizer (dual activity). A non-standardized pharmacological premedication protocol with an H1-receptor antagonist (oxatomide, 0.5 mg/kg) administered 12 hours before the immunizations, and a single dose of betamethasone (0.05 mg/kg) together with another dose of oxatomide (0.5 mg/kg) administered 2 hours before the injections was followed to make it possible for the patient to continue with the scheduled vaccinations. Indeed, no reactions were subsequently reported. Thus, in our experience, a background therapy with ketotifen associated with a premedication protocol made by two doses of oxatomide and a single dose of betamethasone was helpful to make possible the execution of the other vaccines. We suggest how in these children, it could be considered the idea of taking precaution when vaccination is planned, regardless of the kind of vaccine and if a dose of the same vaccine was previously received. However, international consensus needs to be reached to manage vaccinations in children with mastocytosis and previous adverse reactions to vaccines.
疫苗接种是肥大细胞脱颗粒的已知触发因素,在患有肥大细胞增多症的患者中。然而,目前尚无确切的标准化方案来预防疫苗注射后的可能反应,尤其是对于已经出现先前疫苗相关不良事件的患者,因为这些患者通常可以耐受未来的疫苗剂量。出于这个原因,我们旨在分享我们在佛罗伦萨迈耶儿童医院的经验,以提高对未来疫苗接种的潜在风险的认识,并讨论旨在预防这些风险的有价值的治疗策略,同时考虑到文献中专家提出的建议。我们描述了一名 18 个月大的女性患者,患有多形性斑丘疹皮肤肥大细胞增多症,在第二次(加强剂量)灭活四价流感疫苗后 24 小时出现广泛的大疱性皮肤反应,接受了单剂量口服皮质类固醇治疗倍他米松(0.1 毫克/千克)和奥沙他定(1 毫克/千克/天)口服抗组胺治疗一周,直至痊愈。据我们所知,在文献中,没有描述斑丘疹性皮肤肥大细胞增多症对流感疫苗反应的记录病例。随后,患者开始每天服用酮替芬(0.05 毫克/千克,每天两次)、非竞争性 H1 抗组胺药和肥大细胞稳定剂(双重活性)进行背景治疗。在免疫接种前 12 小时给予 H1 受体拮抗剂(奥沙他定,0.5 毫克/千克)和单次剂量的倍他米松(0.05 毫克/千克),并在注射前 2 小时给予另一剂量的奥沙他定(0.5 毫克/千克),制定了一种非标准化的药物预防方案,以便患者能够继续接受计划中的疫苗接种。事实上,随后没有报告任何反应。因此,根据我们的经验,酮替芬联合奥沙他定两剂和倍他米松一剂的背景治疗有助于实施其他疫苗。我们建议在计划疫苗接种时,无论疫苗类型如何,以及之前是否接种过同一疫苗,都可以考虑对这些儿童采取预防措施。然而,需要达成国际共识来管理患有肥大细胞增多症和先前对疫苗有不良反应的儿童的疫苗接种。